Bismuth Subcitrate
JFDA label: Degnol
- Potential for carcinogenicity:
Mechanism of Action
Bismuth: Has both antisecretory and antimicrobial action; may provide some anti-inflammatory action as well. Metronidazole: After diffusing into the organism, interacts with DNA to cause a loss of helical DNA structure and strand breakage resulting in inhibition of protein synthesis and cell death in susceptible organisms. Tetracycline: Inhibits bacterial protein synthesis by binding with the 30S and possibly the 50S ribosomal subunit(s) of susceptible bacteria; may also cause alterations in the cytoplasmic membrane. Bismuth, metronidazole, and tetracycline individually have demonstrated in vitro activity against most susceptible strains of H. pylori isolated from patients with duodenal ulcers.
Indications
Approved
- Duodenal ulcer associated with Helicobacter pylori infection
Contraindications
Source: Lexicomp
- Hypersensitivity (eg, erythema rash, flushing, fever, urticaria) to bismuth, metronidazole, other nitroimidazole derivatives, tetracycline, or any component of the formulation Absolute
- concomitant use with alcohol or other products containing propylene glycol (during therapy and for ≥3 days after) Absolute
- concomitant use with disulfiram (within the previous 2 weeks) Absolute
- concomitant use with methoxyflurane Absolute
- severe renal impairment Absolute
Adverse Reactions
Nervous system disorders (2)
Common dizziness · Headache
Hepatobiliary disorders (2)
Common Increased serum ALT · increased serum AST
Renal and urinary disorders (2)
Common urine abnormality · Vaginitis
Gastrointestinal disorders (7)
Common abdominal pain · constipation · diarrhea · dysgeusia · dyspepsia · Nausea · xerostomia
Skin and subcutaneous tissue disorders (1)
Common Maculopapular rash
Musculoskeletal and connective tissue disorders (1)
Common Weakness
General disorders and administration site conditions (1)
Common Laboratory test abnormality
Other (1)
Very Common Gastrointestinal: Abnormal stools
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
CNS effects
Bismuth may be neurotoxic with excessive doses. Aseptic meningitis (symptoms may occur within hours of a dose), encephalopathy (cerebellar toxicity with ataxia, dizziness, dysarthria, and/or CNS lesions), seizures, peripheral neuropathy (including extremity numbness and paresthesia) and optic neuropathy have been reported with metronidazole. CNS symptoms generally resolve within days to weeks following therapy discontinuation; monitor patients with CNS conditions closely and discontinue promptly if abnormal neurologic signs develop.
Cutaneous reactions
Skin and subcutaneous disorders including Stevens-Johnson, toxic epidermal necrolysis and drug rash with eosinophilia and systemic symptoms (DRESS) have been reported; discontinue treatment at first sign of cutaneous reaction.
Intracranial hypertension
Intracranial hypertension (IH), including pseudotumor cerebri has been reported with use of tetracyclines; women of childbearing age who are overweight or have a history of IH are at greater risk. IH typically resolves after discontinuation of treatment but the possibility for permanent visual loss exists; prompt ophthalmic evaluation is warranted if visual disturbances occur.
Oral/gastrointestinal effects
Bismuth may cause temporary and harmless darkening of the tongue and/or black stools; generally reversible within several days after treatment is discontinued.
Photosensitivity
Tetracycline may cause photosensitivity; avoid exposure to the sun or sun lamps; discontinue use at first evidence of skin erythema.
Potential for carcinogenicity
Metronidazole has been shown to be carcinogenic in mice and rates. It is unknown whether metronidazole is associated with carcinogenicity in humans.
Superinfection
Prolonged use may result in fungal or bacterial superinfection, including C. difficile-associated diarrhea (CDAD) and pseudomembranous colitis; CDAD has been observed >2 months postantibiotic treatment. Disease-related concerns:
Blood dyscrasias
Use metronidazole with caution in patients with or history of blood dyscrasias; mild leukopenia has occurred. Monitor CBC with differential at baseline and after treatment.
Cockayne syndrome
Severe hepatotoxicity/acute hepatic failure (has been fatal) has been reported with systemic metronidazole in patients with Cockayne syndrome; onset is rapid after initiation of treatment. Use metronidazole only after risk vs benefit assessment and if there are no appropriate alternatives in patients with Cockayne syndrome. Obtain LFTs prior to treatment initiation, within the first 2 to 3 days of initiation, frequently during therapy, and after treatment is complete. Discontinue treatment if elevated LFTs occur and monitor until LFTs return to baseline.
Hepatic impairment
Use with caution in patients with mild to moderate hepatic impairment due to potential metronidazole accumulation; use in patients with severe hepatic impairment may not be appropriate.
H. pylori infection
If H. pylori is not eradicated in patients being treated with metronidazole in a regimen, it should be assumed that metronidazole-resistance has occurred and it should not be used again.
Renal impairment
Tetracycline may be associated with increases in BUN secondary to antianabolic effects; use is contraindicated in patients with severe renal impairment. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Pediatric
May cause tissue hyperpigmentation, enamel hypoplasia, or permanent tooth discoloration; more common during long-term treatment, but has been observed following repeated short-term courses. Use of tetracyclines should be avoided during tooth development (children Other warnings/precautions:
Appropriate use
Helicobacter pylori eradication: Short-term combination therapy (≤7 days) has been associated with a higher incidence of treatment failure. The American College of Gastroenterology recommends 10 to 14 days of therapy (triple or quadruple) for eradication of H. pylori (Chey 2017).
Pregnancy & Lactation
Pregnancy
This combination is contraindicated in women who are pregnant. Metronidazole and tetracycline both cross the human placenta and may have adverse effects to the fetus. See individual agents.
Lactation
Metronidazole and tetracycline are excreted in breast milk in concentrations similar to the maternal plasma; it is not known if bismuth is excreted in breast milk. Because of the potential for serious adverse reactions in the nursing infant, the manufacturer recommends that breast-feeding be interrupted during therapy and for 2 days after the last dose. See individual agents.
Monitoring
| Clinical pearl | Monitor CBC with differential at baseline and after treatment (due to metronidazole); development of abnormal neurologic signs/symptoms. H. pylori eradication confirmation, when indicated (Chey, 2007). |
|---|
Chemistry & Properties
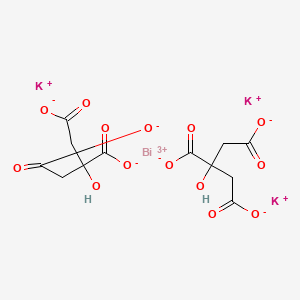
| Formula | C12H13BiO14 |
|---|---|
| Molecular weight | 590.2 g/mol |
| IUPAC name | bismuth;tripotassium;bis(2-hydroxypropane-1,2,3-tricarboxylate) |
| CAS | 57644-54-9 |
| PubChem CID | 10101269 |
Biology & Pharmacokinetics
Pharmacokinetics predicted
| Bioavailability | 70.0% |
|---|---|
| Half-life | 2.138 h |
| Volume of distribution | 0.951 L/kg |
| Protein binding | 10.9% |
| BBB penetrant | No |
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP3A4 | Substrate | — |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)P-gp (Substrate)
Drug–drug interactions (4, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Demeclocycline | moderate | |
| Doxycycline | moderate | |
| Minocycline | moderate | |
| Tetracycline | moderate |
Registered Products (1)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Degnol | Tablet 120 mg | 60 tab | SAVVY PHARMA/JORDAN | 7.970 |