Isoflurane
JFDA label: Floran Anesthetic
Mechanism of Action
Positive Modulator of Glycine receptor (alpha-1/beta) — Glycine receptor (alpha-1/beta) positive modulator; Positive Allosteric Modulator of GABA-A receptor; anion channel — GABA-A receptor; anion channel positive allosteric modulator; Opener of Potassium channel subfamily K member 10 — Potassium channel subfamily K member 10 opener; Opener of Potassium channel subfamily K member 18 — Potassium channel subfamily K member 18 opener; Opener of Potassium channel subfamily K member 3 — Potassium channel subfamily K member 3 opener; Opener of Potassium channel subfamily K member 9 — Potassium channel subfamily K member 9 opener; Opener of Potassium channel subfamily K member 2 — Potassium channel subfamily K member 2 opener
| Target | Action | Gene / class |
|---|---|---|
| GABA-A receptor; anion channel efficacy | POSITIVE ALLOSTERIC MODULATOR | |
| Glycine receptor (alpha-1/beta) efficacy | POSITIVE MODULATOR | |
| Potassium channel subfamily K member 10 efficacy | OPENER | KCNK10 |
| Potassium channel subfamily K member 18 efficacy | OPENER | KCNK18 |
| Potassium channel subfamily K member 2 efficacy | OPENER | KCNK2 |
| Potassium channel subfamily K member 3 efficacy | OPENER | KCNK3 |
| Potassium channel subfamily K member 9 efficacy | OPENER | KCNK9 |
Indications
Approved
- Anesthesia
Contraindications
Source: Lexicomp
- Additional contraindications (not in US labeling): History of hepatitis due to a halogenated inhalational anesthetic or in whom liver dysfunction, jaundice or unexplained fever, leucocytosis, or eosinophilia has occurred after a previous halogenated anesthetic administration Absolute
- Known sensitivity to isoflurane, other halogenated agents, or any component of the formulation Absolute
- known or suspected genetic susceptibility to malignant hyperthermia Absolute
- patients in whom general anesthesia is contraindicated Absolute
Adverse Reactions
Cardiac disorders (4)
Not Known Cardiac arrhythmia · cardiac insufficiency · hypotension · tachycardia (transient)
Nervous system disorders (4)
Not Known Cognitive dysfunction (may persist for ≤3 days after administration) · malignant hyperthermia · mood changes (may persist for ≤6 days after administration) · shivering
Hepatobiliary disorders (1)
Not Known Decreased alkaline phosphatase
Renal and urinary disorders (1)
Not Known Increased serum creatinine
Blood and lymphatic system disorders (1)
Not Known Leukocytosis (transient)
Metabolism and nutrition disorders (4)
Not Known Decreased blood urea nitrogen · decreased serum cholesterol · hyperglycemia · hyperkalemia (perioperative)
Gastrointestinal disorders (3)
Not Known Intestinal obstruction · nausea · vomiting
Musculoskeletal and connective tissue disorders (1)
Not Known Laryngospasm (related to induction)
Respiratory, thoracic and mediastinal disorders (2)
Not Known Cough (related to induction) · respiratory depression
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Cardiovascular effects
Decrease in blood pressure is dose dependent due to peripheral vasodilation; cardiac output is maintained. Use caution in patients who are hypovolemic, hypotensive, or hemodynamically compromised; use caution in patients with coronary artery disease to avoid risk of myocardial ischemia. May prolong the QT interval and rarely torsades de pointes; use caution in patients at risk of QT prolongation. May produce cardiac steal (due to coronary vasodilation) and reflex tachycardia, but does not depress cardiac conduction nor does it sensitize the myocardium to catecholamine-induced arrhythmias like halothane (not available in the United States) (Golembiewski 2004).
Decreased blood flow
May cause decrease in hepatic, renal, and splenic blood flow (Gelman 1984).
Hepatic effects
Postoperative mild to severe hepatic dysfunction (some fatal) and hepatitis have been reported; may cause sensitivity hepatitis in patients who have been sensitized by previous exposure to halogenated anesthetics.
Hyperkalemia
Use of inhaled anesthetics has been associated with rare cases of perioperative hyperkalemia that have resulted in cardiac arrhythmias (including fatalities) in pediatric patients; concomitant use of succinylcholine was associated with many of the reported cases, but not all. Risk of hyperkalemia is increased in pediatric patients with underlying neuromuscular disease (eg, Duchenne muscular dystrophy). Other abnormalities may include elevation in creatinine kinase (CK) and myoglobinuria. Monitor closely for hyperkalemic-associated arrhythmias; aggressively identify and treat.
Increased intracranial pressure
Dilates the cerebral vasculature and may, in certain conditions, increase intracranial pressure.
Malignant hyperthermia
May trigger malignant hyperthermia; use is contraindicated in patients susceptible to malignant hyperthermia.
Obstetrical anesthesia
Increased blood loss comparable with that seen with halothane has been reported during abortions.
Respiratory depression
Causes dose-dependent respiratory depression and blunted ventilatory response to hypoxia and hypercapnia (Golembiewski 2004). Disease-related concerns:
Heart failure
In a scientific statement from the American Heart Association, isoflurane has been determined to be an agent that may exacerbate underlying myocardial dysfunction (magnitude: major) (AHA [Page 2016]). Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Pediatric neurotoxicity
In pediatric and neonatal patients Special handling:
Occupational caution
There is no specific work exposure limit established for isoflurane. However, the National Institute for Occupational Safety and Health (NIOSH) recommends no worker be exposed to >2 ppm (ceiling concentrations) over a period of 1 hour. Precautions (eg, adequate ventilation, scavenging-systems, minimizing leaks/spills) can help to lessen any potential risk. Other warnings/precautions:
Desiccated absorbents
Reaction of isoflurane with desiccated CO2 absorbents produce carbon monoxide, which may result in elevated carboxyhemoglobin levels in some patients.
Pregnancy & Lactation
Pregnancy
Adverse events have been observed in animal reproduction studies. Based on animal data, repeated or prolonged use of general anesthetic and sedation medications that block N-methyl-D- aspartate (NMDA) receptors and/or potentiate gamma-aminobutyric acid (GABA) activity, may affect brain development. Human fetuses may be most vulnerable during the third trimester. Until additional information is available, the benefits and risks of maternal treatment with isoflurane during pregnancy should be evaluated, especially for procedures lasting more than 3 hours. The ACOG recommends that pregnant women should not be denied medically indicated surgery or procedures, regardless of trimester. If the procedure is elective, it should be delayed until after delivery (ACOG 2011).
Lactation
It is not known if isoflurane is present in breast milk. The manufacturer recommends that caution be exercised when administering isoflurane to breastfeeding women.
Monitoring
| Clinical pearl | Blood pressure, heart rate and rhythm, serum potassium, oxygen saturation, end-tidal CO2 and isoflurane concentrations should be monitored prior to and throughout anesthesia |
|---|
Chemistry & Properties
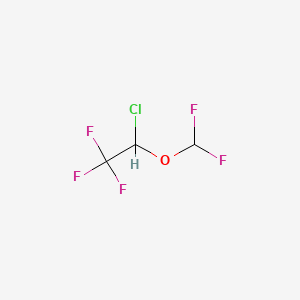
| Formula | C3H2ClF5O |
|---|---|
| Molecular weight | 184.49 g/mol |
| IUPAC name | 2-chloro-2-(difluoromethoxy)-1,1,1-trifluoroethane |
| CAS | 26675-46-7 |
| PubChem CID | 3763 |
| InChIKey | PIWKPBJCKXDKJR-UHFFFAOYSA-N |
| logP | 2.35 (XLogP 2.1) |
| Polar surface area | 9.23 Ų |
| H-bond acceptors / donors | 1 / 0 |
| Drug-likeness (QED) | 0.47 |
| Lipinski violations | 0 |
SMILES
FC(F)OC(Cl)C(F)(F)FBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | Yes (logBB 0.42) |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP1A2 | Substrate | — |
| CYP2B6 | Substrate | — |
| CYP2C19 | Substrate | — |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)P-gp (Substrate)
Drug–drug interactions (7, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Epinephrine | major | |
| Ceritinib | moderate | |
| Codeine | moderate | |
| Doxepin | moderate | |
| Hydrocodone | moderate | |
| Morphine | moderate | |
| Opium | moderate |
Registered Products (3)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Aerrane | Solution 100 % | 100 ml pack varies | Khoury Drug Store | — |
| Aerrane | Solution 100 % | 250 ml pack varies | Khoury Drug Store | — |
| Floran Anesthetic | Solution 100 % | 100 ml | Hikma Pharmaceuticals Co.Ltd/Jordan | — |