Amikacin
🧬 Cross-allergy: Aminoglycosides
JFDA label: Likacin Inj
- Ototoxicity:
- Nephrotoxicity:
- Neuromuscular blockade:
- Monitoring:
- Concurrent therapy:
- Nephrotoxicity
Mechanism of Action
Inhibits protein synthesis in susceptible bacteria by binding to 30S ribosomal subunits
Indications
Approved
- Serious infections
Off-label
- Bacterial endophthalmitis
- Cystic fibrosis exacerbation (aerosolized amikacin)
- Mycobacterium avium complex (MAC)
- Tuberculosis
Antimicrobial Spectrum
Expected / intrinsic spectrum (EUCAST breakpoints & labels) — not local resistance. Source: EUCAST v16 · curated · openfda-label.
Bacteria
| Organism | Activity | MIC |
|---|---|---|
| Acinetobacter baumannii | Susceptible | 8.0 mg/L |
| Acinetobacter spp. | Susceptible | 81.0 mg/L |
| Citrobacter freundii | Active | — |
| Enterobacterales | Susceptible | 81.0 mg/L |
| Escherichia coli | Susceptible | 8.0 mg/L |
| Klebsiella pneumoniae | Susceptible | 8.0 mg/L |
| Mycobacterium tuberculosis | Susceptible | 1.0 mg/L |
| Proteus rettgeri | Active | — |
| Providencia stuartii | Active | — |
| Pseudomonas aeruginosa | Susceptible | 8.0 mg/L |
| Pseudomonas aeruginosa | Susceptible | 161.0 mg/L |
| Serratia marcescens | Active | — |
| Acinetobacter baumannii | Resistant | 16.0 mg/L |
| Escherichia coli | Resistant | 16.0 mg/L |
| Klebsiella pneumoniae | Resistant | 16.0 mg/L |
| Pseudomonas aeruginosa | Resistant | 16.0 mg/L |
Class profile
| gramStatus | Both |
|---|---|
| spectrumBreadth | Moderate |
| atypicalCoverage | No |
| isBactericidal | 1 |
| moaCategory | Protein synthesis inhibitor (30S ribosomal) |
| pdIndex | Concentration-dependent |
| postAntibioticEffect | Prolonged |
| mrsaCoverage | 0 |
| resistanceMechanisms | Aminoglycoside-modifying enzymes,Ribosomal methylation (16S rRNA),Reduced outer membrane permeability |
Contraindications
Source: Lexicomp
- Hypersensitivity to amikacin, other aminoglycosides, or any component of the formulation Absolute
Adverse Reactions
Nervous system disorders (1)
Common Neurotoxicity
Ear and labyrinth disorders (2)
Common Auditory ototoxicity · vestibular ototoxicity
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Hypersensitivity
Cross-sensitivity to other aminoglycosides may occur.
Nephrotoxicity
May cause nephrotoxicity; usual risk factors include preexisting renal impairment, concomitant nephrotoxic medications, advanced age and dehydration. Discontinue treatment if signs of nephrotoxicity occur; renal damage is usually reversible.
Neuromuscular blockade and respiratory paralysis
May cause neuromuscular blockade and respiratory paralysis; especially when given soon after anesthesia or muscle relaxants.
Neurotoxicity
May cause neurotoxicity; usual risk factors include preexisting renal impairment, concomitant neuro-/nephrotoxic medications, advanced age and dehydration. Ototoxicity is proportional to the amount of drug given and the duration of treatment. Tinnitus or vertigo may be indications of vestibular injury and impending bilateral irreversible damage. Discontinue treatment if signs of ototoxicity occur.
Superinfection
Prolonged use may result in fungal or bacterial superinfection, including C. difficile-associated diarrhea (CDAD) and pseudomembranous colitis; CDAD has been observed >2 months postantibiotic treatment. Disease-related concerns:
Hearing impairment
Use with caution in patients with preexisting vertigo, tinnitus, or hearing loss.
Hypocalcemia
Use with caution in patients with hypocalcemia.
Neuromuscular disorders
Use with caution in patients with neuromuscular disorders, including myasthenia gravis or parkinsonism.
Renal impairment
Use with caution in patients with preexisting renal insufficiency; dosage modification required. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
Neurotoxic and/or nephrotoxic drugs
Avoid concomitant or sequential use of other neurotoxic and/or nephrotoxic drugs (eg, bacitracin, cisplatin, amphotericin B, paromomycin, polymyxin B, colistin, vancomycin, other aminoglycosides).
Potent diuretics
Avoid concomitant use with potent diuretics (eg, ethacrynic acid, furosemide) since diuretics themselves may cause ototoxicity and may enhance aminoglycoside toxicity. Dosage form specific issues:
Sulfites
May contain sulfites which may cause allergic-type reactions (including anaphylaxis) as well as life-threatening or less severe asthmatic episodes in certain individuals. Other warnings/precautions:
Surgical irrigation
Irreversible deafness, renal failure, and death due to neuromuscular blockade have been reported following use of aminoglycosides as surgical irrigation; rapid systemic absorption occurs with topical application (except to the urinary bladder).
Pregnancy & Lactation
Pregnancy
Adverse events were not observed in the initial animal reproduction studies. Amikacin crosses the placenta and produces detectable concentrations in the fetus. Aminoglycosides may cause fetal harm if administered to a pregnant woman. There are several reports of total irreversible bilateral congenital deafness in children whose mothers received another aminoglycoside (streptomycin) during pregnancy. Although serious side effects to the fetus/infant have not been reported following maternal use of all aminoglycosides, a potential for harm exists. Due to pregnancy-induced physiologic changes, some pharmacokinetic parameters of amikacin may be altered (Bernard 1977).
Lactation
Amikacin is excreted into breast milk (trace amounts) (Matsuda 1984). Due to the potential for serious adverse reactions in the nursing infant, the manufacturer recommends a decision be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of treatment to the mother. As a class, aminoglycosides are expected to be poorly distributed into breast milk, limiting systemic exposure to a nursing infant. In general, modification of bowel flora may occur with
LactMed: monitor the infant.
Monitoring
| Efficacy | Peak 20–30 mg/L (30 min post-infusion); trough < 5 mg/L (once-daily: trough < 1 mg/L); renal function; audiogram for prolonged therapy |
|---|---|
| Toxicity | Nephrotoxicity; ototoxicity (auditory and vestibular); check SCr every 2–3 days in at-risk patients |
| Clinical pearl | Like gentamicin but used for resistant organisms including MDR-TB. AUC-guided dosing is increasingly preferred. |
| Counseling | Report hearing changes, dizziness, or decreased urination immediately. |
Chemistry & Properties
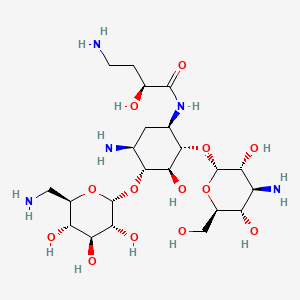
| Formula | C22H43N5O13 |
|---|---|
| Molecular weight | 585.61 g/mol |
| IUPAC name | (2S)-4-amino-N-[(1R,2S,3S,4R,5S)-5-amino-2-[(2S,3R,4S,5S,6R)-4-amino-3,5-dihydroxy-6-(hydroxymethyl)oxan-2-yl]oxy-4-[(2R,3R,4S,5S,6R)-6-(aminomethyl)-3,4,5-trihydroxyoxan-2-yl]oxy-3-hydroxycyclohexyl]-2-hydroxybutanamide |
| CAS | 37517-28-5 |
| PubChem CID | 37768 |
| InChIKey | LKCWBDHBTVXHDL-RMDFUYIESA-N |
| logP | -8.42 (XLogP -7.9) |
| Polar surface area | 331.94 Ų |
| H-bond acceptors / donors | 17 / 13 |
| Drug-likeness (QED) | 0.11 |
| Lipinski violations | 3 |
SMILES
NCC[C@H](O)C(=O)N[C@@H]1C[C@H](N)[C@@H](O[C@H]2O[C@H](CN)[C@@H](O)[C@H](O)[C@H]2O)[C@H](O)[C@H]1O[C@H]1O[C@H](CO)[C@@H](O)[C@H](N)[C@H]1OBiology & Pharmacokinetics
Pharmacokinetics predicted
| Bioavailability | 70.0% |
|---|---|
| Half-life | 2.921 h |
| Volume of distribution | 0.2 L/kg |
| Protein binding | 10.9% |
| BBB penetrant | No |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Atracurium | major | |
| Bacitracin | major | |
| Botulinum Toxin Type B | major | |
| Botulinum toxin type A | major | |
| Bumetanide | major | |
| Capreomycin | major | |
| Cidofovir | major | |
| Cisatracurium | major | |
| Colistimethate | major | |
| Deferasirox | major | |
| Diatrizoate | major | |
| Doxacurium | major | |
| Etacrynic acid | major | |
| Everolimus | major | |
| Foscarnet | major | |
| Furosemide | major | |
| Gallium nitrate | major | |
| Human Rho(D) immune globulin | major | |
| Human botulinum neurotoxin A/B immune globulin | major | |
| Human cytomegalovirus immune globulin | major | |
| Human immunoglobulin G (intravenous and subcutaneous) | major | |
| Human immunoglobulin G (intravenous) | major | |
| Inotersen | major | |
| Iodipamide | major | |
| Iodixanol | major | |
| Iohexol | major | |
| Iopamidol | major | |
| Iopromide | major | |
| Iothalamic acid | major | |
| Ioversol | major | |
| Ioxilan | major | |
| Magnesium sulfate | major | |
| Mannitol | major | |
| Metocurine | major | |
| Mivacurium | major | |
| Pancuronium | major | |
| Pipecuronium | major | |
| Polymyxin B | major | |
| Rapacuronium | major | |
| Rocuronium | major |
Showing 40 of 100+.
Registered Products (11)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Amiswiss | Vial 500 mg/2 ml | 1 vial | Argon drug store | 0.460 |
| Likacin Inj | Injection 500 mg/2 ml | 1 vial pack varies | AL Rahma Drug Store | 3.480 |
| Likacin Gel | Gel 5 % | 30 g tube | AL Rahma Drug Store | 4.620 |
| Miacin 100 Ampoules | Ampoule (as Sulphate) 100 mg/2 ml | 6 amp | Hikma Pharmaceuticals Co.Ltd/Jordan | 4.930 |
| Amicine 250mg/2ml Solution for Inj | Injection 250 mg/2 ml | 5 vial | MS PHARMA/JORDAN | 18.610 |
| Amicine 500mg/2ml Solution for Inj | Injection 500 mg/2 ml | 5 vial | MS PHARMA/JORDAN | 18.610 |
| Miacin 500 Ampoules | Ampoule 500 mg/2 ml | 6 amp | Hikma Pharmaceuticals Co.Ltd/Jordan | 24.000 |
| Selemycin | Ampoule 250 mg/2 ml | 10 amp | Al Hilal Drug Store | 27.680 |
| Selemycin | Ampoule 500 mg/2 ml | 10 amp | Al Hilal Drug Store | 45.200 |
| Likacin Inj | Injection 500 mg/2 ml | 50 vial pack varies | AL Rahma Drug Store | 147.900 |
| Amikam | Vial 250 mg/ml | 2 ml | ٠ستÙدع أدÙÙØ© اÙÙÙÙÙÙÙ | — |