Deferoxamine
JFDA label: Noferal
Mechanism of Action
Complexes with trivalent ions (ferric ions), primarily in the vascular space, to form ferrioxamine, which is eliminated in the urine by the kidneys. One hundred milligrams of deferoxamine will bind about 8.5 mg of free circulating elemental iron (85 mg per 1,000 mg dose) but does not remove iron from transferrin or hemoglobin. Binding of cytoplasmic free iron reduces the free iron-induced disruption of mitochondrial cell membranes and enzyme systems. Ferrioxamine may create a pink- to red- or orange-colored urine as it is being excreted.
Indications
Approved
- Acute iron toxicity
- Chronic iron overload
Off-label
- Diagnosis or treatment of aluminum-induced toxicity associated with chronic kidney disease (CKD)
Contraindications
Source: Lexicomp
- Hypersensitivity to deferoxamine or any component of the formulation Absolute
- patients with severe renal disease or anuria Absolute
Adverse Reactions
Cardiac disorders (4)
Not Known Flushing · hypotension · shock · tachycardia
Nervous system disorders (6)
Not Known Brain disease (aluminum toxicity/dialysis-related) · dizziness · headache · neuropathy (peripheral, sensory, motor, or mixed) · paresthesia · seizure
Renal and urinary disorders (5)
Not Known Acute renal failure · Dysuria · increased serum creatinine · renal tubular disease · urine discoloration (reddish color)
Blood and lymphatic system disorders (1)
Not Known Dysplasia (metaphyseal; children Hepatic: Hepatic insufficiency, increased serum transaminases
Immune system disorders (3)
Not Known Anaphylaxis (with or without shock) · angioedema · hypersensitivity
Metabolism and nutrition disorders (3)
Not Known Growth suppression (children) · hyperparathyroidism (aggravated) · hypocalcemia
Gastrointestinal disorders (5)
Not Known Abdominal distress · abdominal pain · diarrhea · nausea · vomiting
Skin and subcutaneous tissue disorders (2)
Not Known Skin rash · urticaria
Musculoskeletal and connective tissue disorders (3)
Not Known Arthralgia · muscle spasm · myalgia
Eye disorders (12)
Not Known Blurred vision · cataract · chromatopsia · corneal opacity · decreased peripheral vision · decreased visual acuity · nocturnal amblyopia · optic neuritis · retinal pigment changes · scotoma · vision loss · visual field defect
Ear and labyrinth disorders (2)
Not Known Hearing loss · tinnitus
Infections and infestations (1)
Not Known Infection (Yersinia, mucormycosis)
General disorders and administration site conditions (2)
Not Known Fever · Injection site reaction (burning, crust, edema, erythema, eschar, induration, infiltration, irritation, pain, pruritus, swelling, vesicles, wheal formation)
Respiratory, thoracic and mediastinal disorders (2)
Not Known Acute respiratory distress (dyspnea, cyanosis, and/or interstitial infiltrates) · asthma
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Acute respiratory distress syndrome (ARDS)
Deferoxamine has been associated with ARDS following excessively high-dose IV treatment of acute iron intoxication or thalassemia; has been reported in children and adults.
Auditory effects
Auditory disturbances (tinnitus and high frequency hearing loss) have been reported following prolonged administration, at high doses, or in patients with low ferritin levels; effects are generally reversible with early detection and immediate discontinuation. Elderly patients are at increased risk for hearing loss. Audiology exams are recommended with long-term treatment.
Growth retardation
High deferoxamine doses and concurrent low ferritin levels are also associated with growth retardation. Growth velocity may partially resume to pretreatment rates after deferoxamine dose reduction.
Infection
Patients with iron overload are at increased susceptibility to infection with Yersinia enterocolitica and Yersinia pseudotuberculosis; treatment with deferoxamine may enhance this risk; if infection develops, discontinue therapy until resolved.
Infusion reactions
Flushing of the skin, hypotension, urticaria, and shock are associated with rapid IV infusion; administer by slow IV infusion, IM, or slow subcutaneous infusion only.
Mucormycosis
Rare and serious cases of mucormycosis (including fatalities) have been reported with use; withhold treatment with signs and symptoms of mucormycosis.
Ocular effects
Ocular disturbances (blurred vision; cataracts; corneal opacities; decreased visual acuity; impaired peripheral, color, and night vision; optic neuritis; retinal pigment abnormalities; retinopathy; scotoma; visual loss/defect) have been reported following prolonged administration, at high doses, or in patients with low ferritin levels; effects are generally reversible with early detection and immediate discontinuation. Elderly patients are at increased risk for ocular disorders. Periodic ophthalmic exams are recommended with long-term treatment.
Renal effects
Increases in serum creatinine, acute renal failure and renal tubular disorders have been reported; monitor for changes in renal function. Deferoxamine is readily dialyzable. When iron is chelated with deferoxamine, the chelate is water-soluble and is excreted renally.
Urine discoloration
Patients should be informed that urine may have a pink, reddish, or orange discoloration. Disease-related concerns:
Aluminum toxicity
Treatment with deferoxamine in patients with aluminum toxicity may cause hypocalcemia and aggravate hyperparathyroidism. Deferoxamine may cause neurological symptoms (including seizure) in patients with aluminum-related encephalopathy receiving dialysis and may precipitate dialysis dementia onset.
Hemochromatosis
Deferoxamine is not indicated for the treatment of primary hemochromatosis (treatment of choice is phlebotomy). Concurrent drug therapy issues:
Ascorbic acid
Combination treatment with ascorbic acid (>500 mg/day in adults) and deferoxamine may impair cardiac function (rare), effects are reversible upon discontinuation of ascorbic acid. If combination treatment is warranted, initiate ascorbic acid only after one month of regular deferoxamine treatment, do not exceed ascorbic acid dose of 200 mg/day for adults (in divided doses), 100 mg/day for children ≥10 years of age, or 50 mg/day in children
Pregnancy & Lactation
Pregnancy
Adverse events have been observed in animal reproduction studies. Toxic amounts of iron or deferoxamine have not been noted to cross the placenta; however, the metabolic effects of a maternal overdose may adversely affect the fetus. In case of acute iron toxicity, treatment during pregnancy should not be withheld (Chang 2011).
Lactation
It is not known if deferoxamine is excreted in breast milk. The manufacturer recommends that caution be exercised when administering to nursing women.
Monitoring
| Clinical pearl | Serum iron, ferritin, total iron-binding capacity, CBC with differential, renal function tests (serum creatinine), liver function tests, serum chemistries; ophthalmologic exam (visual acuity tests, fundoscopy, slit-lamp exam) and audiometry with long-term treatment; growth and body weight in children (every 3 months). When deferoxamine complexes with iron it forms a water-soluble compound (ferrixoamine) that imparts discoloration of the urine; often described as vin rosé (dark pink) discoloration to the urine (Fernández 2014). However, other than being aware of that it may occur, its presence or absence should not be used as a therapeutic endpoint. Dialysis patients: Serum aluminum (yearly; every 3 months in patients on aluminum-containing medications) Aluminum-induced bone disease: Serum aluminum concentration 2 days following deferoxamine test dose; test is considered positive if the serum aluminum increases ≥50 mcg/L |
|---|
Chemistry & Properties
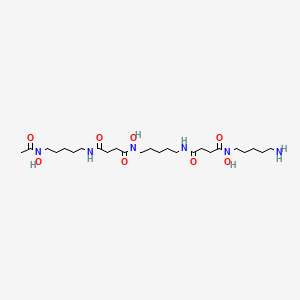
| Formula | C25H48N6O8 |
|---|---|
| Molecular weight | 560.69 g/mol |
| IUPAC name | N-[5-[[4-[5-[acetyl(hydroxy)amino]pentylamino]-4-oxobutanoyl]-hydroxyamino]pentyl]-N'-(5-aminopentyl)-N'-hydroxybutanediamide |
| CAS | 70-51-9 |
| PubChem CID | 2973 |
| InChIKey | UBQYURCVBFRUQT-UHFFFAOYSA-N |
| logP | 0.92 (XLogP -2.1) |
| Polar surface area | 205.84 Ų |
| H-bond acceptors / donors | 9 / 6 |
| Drug-likeness (QED) | 0.06 |
| Lipinski violations | 2 |
SMILES
CC(=O)N(O)CCCCCNC(=O)CCC(=O)N(O)CCCCCNC(=O)CCC(=O)N(O)CCCCCNBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2C19 | Substrate | — |
| CYP3A4 | Inhibitor | — |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)P-gp (Substrate)
Drug–drug interactions (18, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Cidofovir | major | |
| Diatrizoate | major | |
| Inotersen | major | |
| Iodipamide | major | |
| Iodixanol | major | |
| Iohexol | major | |
| Iopamidol | major | |
| Iopromide | major | |
| Iothalamic acid | major | |
| Ioversol | major | |
| Ioxilan | major | |
| Vigabatrin | major | |
| Ascorbic acid | moderate | |
| Busulfan | moderate | |
| Clofarabine | moderate | |
| Gallium chloride Ga-67 | moderate | |
| Prochlorperazine | moderate | |
| Remdesivir | moderate |
Registered Products (2)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Froxa | Vial 500 mg | 10 vial | MS PHARMA/JORDAN | — |
| Noferal | Vial 500 mg | 10 vial | Hikma Pharmaceuticals Co.Ltd/Jordan | — |