Imipenem
🧬 Cross-allergy: Carbapenems
JFDA label: Premax 500mg/500mg
Mechanism of Action
Inhibitor of Bacterial penicillin-binding protein — Bacterial penicillin-binding protein inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Bacterial penicillin-binding protein efficacy | INHIBITOR |
Indications
Approved
- Bacterial septicemia
- Bone and joint infections
- Endocarditis
- Gynecologic infections
- Intra-abdominal infections
- Lower respiratory tract infections
- Skin and skin structure infections
- Urinary tract infections (complicated and uncomplicated)
Off-label
- Burkholderia pseudomallei (melioidosis)
- Cystic fibrosis exacerbations (children and adolescents)
- Neutropenic fever
- Nontuberculous mycobacterial disease
- Skin and soft tissue necrotizing infections
- Surgical-site infection
Antimicrobial Spectrum
Expected / intrinsic spectrum (EUCAST breakpoints & labels) — not local resistance. Source: EUCAST v16 · curated · openfda-label.
Bacteria
| Organism | Activity | MIC |
|---|---|---|
| Acinetobacter baumannii | Susceptible | 2.0 mg/L |
| Acinetobacter calcoaceticus | Active | — |
| Acinetobacter spp. | Susceptible | 2.0 mg/L |
| Anaerobes | Susceptible | 1.0 mg/L |
| Bacillus spp. | Susceptible | 0.5 mg/L |
| Bacteroides caccae | Active | — |
| Bacteroides fragilis | Active | — |
| Bacteroides ovatus | Active | — |
| Bacteroides stercoris | Active | — |
| Bacteroides thetaiotaomicron | Active | — |
| Bacteroides uniformis | Active | — |
| Bacteroides vulgatus | Active | — |
| Citrobacter freundii | Active | — |
| Citrobacter koseri | Active | — |
| Enterobacter asburiae | Active | — |
| Enterobacter cloacae | Susceptible | 2.0 mg/L |
| Enterococcus faecalis | Active | — |
| Enterococcus faecium | Active | — |
| Escherichia coli | Susceptible | 2.0 mg/L |
| Fusobacterium necrophorum | Active | — |
| Fusobacterium nucleatum | Active | — |
| Fusobacterium varium | Active | — |
| Haemophilus influenzae | Susceptible | 2.0 mg/L |
| Klebsiella aerogenes | Active | — |
| Klebsiella oxytoca | Active | — |
| Klebsiella pneumoniae | Susceptible | 2.0 mg/L |
| Moraxella catarrhalis | Susceptible | 2.0 mg/L |
| Peptostreptococcus anaerobius | Active | — |
| Prevotella bivia | Active | — |
| Pseudomonas aeruginosa | Susceptible | 4.0 mg/L |
| Pseudomonas aeruginosa | Susceptible | 0.001 mg/L |
| Serratia marcescens | Active | — |
| Staphylococcus aureus | Active | — |
| Streptococcus anginosus | Active | — |
| Streptococcus constellatus | Active | — |
| Streptococcus pneumoniae | Susceptible | 2.0 mg/L |
| Viridans group streptococci | Susceptible | 2.0 mg/L |
| Acinetobacter baumannii | Resistant | 8.0 mg/L |
| Escherichia coli | Resistant | 8.0 mg/L |
| Klebsiella pneumoniae | Resistant | 8.0 mg/L |
| Pseudomonas aeruginosa | Resistant | 8.0 mg/L |
| Stenotrophomonas maltophilia | Resistant | 4.0 mg/L |
Class profile
| gramStatus | Both |
|---|---|
| spectrumBreadth | Extended |
| atypicalCoverage | No |
| isBactericidal | 1 |
| moaCategory | Cell wall synthesis inhibitor (beta-lactam, carbapenem) |
| pdIndex | Time-dependent |
| postAntibioticEffect | Short |
| mrsaCoverage | 0 |
| resistanceMechanisms | Carbapenemase (KPC,NDM,OXA-48),OprD porin loss,Efflux pumps |
Contraindications
Source: Lexicomp
- Hypersensitivity to imipenem/cilastatin or any component of the formulation Documentation of allergenic cross-reactivity for carbapenems, penicillins, and cephalosporins is limited. However, because of similarities in chemical structure and/or pharmacologic actions, the possibility of cross-sensitivity cannot be ruled out with certainty Absolute
Adverse Reactions
Cardiac disorders (2)
Very Common Phlebitis · tachycardia
Renal and urinary disorders (4)
Very Common Increased serum creatinine (neonates and infants Clostridium difficile associated diarrhea, confusion, cyanosis, decreased serum sodium, dental discoloration, dizziness, drowsiness, drug fever, dysgeu · oliguria · Proteinuria · urine discoloration
Blood and lymphatic system disorders (1)
Very Common Decreased hematocrit (infants and children 3 months to 12 years: 18%; neonates and infants Hepatic: Increased serum AST (infants and children 3 months to 12 years: 18%; neonates and infants 1% to 10%:
Gastrointestinal disorders (5)
Very Common Diarrhea · gastroenteritis · nausea · oral candidiasis · vomiting
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
CNS effects
Carbapenems have been associated with CNS adverse effects, including confusional states and seizures (myoclonic); use caution with CNS disorders (eg, brain lesions and history of seizures) and adjust dose in renal impairment to avoid drug accumulation, which may increase seizure risk. However, there have been reports of adverse CNS effects in patients who had no recognized or documented underlying CNS disorder or compromised renal function.
Hypersensitivity reactions
Serious hypersensitivity/anaphylactic reactions have been reported, including fatalities; may be more common in patients with a history of sensitivity to multiple allergens. Patients with a history of penicillin hypersensitivity may experience severe hypersensitivity reactions when treated with other beta-lactams; carefully inquire about previous hypersensitivity reactions to penicillins, cephalosporins, other beta-lactams, and other allergens. Serious anaphylactic reactions require immediate discontinuation and supportive care as clinically indicated.
Superinfection
Prolonged use may result in fungal or bacterial superinfection, including C. difficile-associated diarrhea (CDAD) and pseudomembranous colitis; CDAD has been observed >2 months postantibiotic treatment. Disease-related concerns:
Renal impairment
Use with caution in patients with renal impairment; dosage adjustment required in patients with moderate to severe renal dysfunction. Increased seizure risk has been reported in patients with significant renal dysfunction. Do not use in patients with CrCl ≤15 mL/minute unless hemodialysis is instituted within 48 hours. For patients on hemodialysis, use is recommended only when the benefit outweighs the potential risk of seizures. Concurrent drug therapy issues:
Valproic acid and derivatives
Carbapenems, including imipenem, may decrease the serum concentration of divalproex sodium/valproic acid increasing the risk of breakthrough seizures. Concurrent use of carbapenem antibiotics with divalproex sodium/valproic acid is generally not recommended. Alternative antimicrobial agents should be considered, but if a concurrent carbapenem is necessary, consider additional antiseizure medication.
Drug-drug interactions
Additional potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Pediatric
Not recommended in pediatric CNS infections due to seizure potential. Not recommended in pediatric patients
Pregnancy & Lactation
Pregnancy
Adverse events have not been observed in animal reproduction studies. Due to pregnancy induced physiologic changes, some pharmacokinetic parameters of imipenem/cilastatin may be altered. Pregnant women have a larger volume of distribution resulting in lower serum peak levels than for the same dose in nonpregnant women. Clearance is also increased.
Lactation
Imipenem is excreted in human milk. The low concentrations and low oral bioavailability suggest minimal exposure risk to the infant. The US labeling recommends that caution be exercised when administering imipenem/cilastatin to breast-feeding women. The Canadian labeling recommends discontinuing breast-feeding if therapy is considered necessary. Nondose-related effects could include modification of bowel flora.
Monitoring
| Efficacy | Culture and susceptibility testing; clinical resolution (temperature, WBC, CRP, procalcitonin) |
|---|---|
| Toxicity | Renal function (dose adjustment in renal impairment); hepatic function for hepatically cleared agents; signs of C. difficile infection (diarrhoea) |
| Clinical pearl | Culture results guide de-escalation to narrower-spectrum therapy. Review antibiotic appropriateness at 48–72 h (antimicrobial stewardship). |
| Counseling | Complete the full course. Report persistent diarrhoea, rash, or lack of improvement after 48–72 h. |
Chemistry & Properties
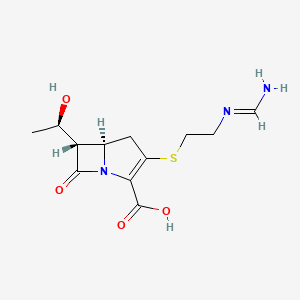
| Formula | C12H19N3O5S |
|---|---|
| Molecular weight | 317.37 g/mol |
| IUPAC name | (5R,6S)-3-[2-(aminomethylideneamino)ethylsulfanyl]-6-[(1R)-1-hydroxyethyl]-7-oxo-1-azabicyclo[3.2.0]hept-2-ene-2-carboxylic acid |
| CAS | 64221-86-9 |
| PubChem CID | 104838 |
| InChIKey | GSOSVVULSKVSLQ-JJVRHELESA-N |
| logP | -0.18 (XLogP -0.7) |
| Polar surface area | 113.72 Ų |
| H-bond acceptors / donors | 5 / 4 |
| Drug-likeness (QED) | 0.22 |
| Lipinski violations | 0 |
SMILES
C[C@@H](O)[C@H]1C(=O)N2C(C(=O)O)=C(SCCNC=N)C[C@H]12.OBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2B6 | Inhibitor | — |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)MRP4 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)P-gp (Substrate)
Drug–drug interactions (15, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Bupropion | major | |
| Iohexol | major | |
| Iopamidol | major | |
| Aminophylline | moderate | |
| Cyclosporine | moderate | |
| Dicoumarol | moderate | |
| Dyphylline | moderate | |
| Ethinylestradiol | moderate | |
| Lindane | moderate | |
| Mycophenolic acid | moderate | |
| Oxtriphylline | moderate | |
| Pemetrexed | moderate | |
| Polyethylene glycol (3350 with electrolytes) | moderate | |
| Theophylline | moderate | |
| Warfarin | moderate |
Registered Products (7)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Cilanem | Vial 500 mg, 500 mg | 1 vial | Reda Jardaneh Drug Store | — |
| Imista( 500mg+500mg) powder for solution for infusion | Infusion 500 mg, 500 mg | 10 vial | ORIENT DRUG STORE CO | — |
| Ivnem | Vial 500 mg, 500 mg | 10 vial | The Arab Pharmaceutical Manufactruing Co | — |
| Premax 500mg/500mg | Vial 500 mg, 500 mg | 1 vial pack varies | Al-Taqqadom Pharmaceutical Industries | — |
| Premax 500mg/500mg | Vial 500 mg, 500 mg | 50 vial pack varies | Al-Taqqadom Pharmaceutical Industries | — |
| Premax 500mg/500mg | Vial 500 mg, 500 mg | 10 vial pack varies | Al-Taqqadom Pharmaceutical Industries | — |
| Tienam for IV Infusion | Infusion 500 mg, 500 mg | 1 vial | Adatco Drug Store | — |