Sofosbuvir
Active form: Gs-461203.
JFDA label: Harvoni 90mg /400mg
- Hepatitis B virus reactivation:
Mechanism of Action
Inhibitor of RNA-directed RNA polymerase — RNA-directed RNA polymerase inhibitor
| Target | Action | Gene / class |
|---|---|---|
| RNA-directed RNA polymerase efficacy | INHIBITOR | NS5b |
Indications
Approved
- Chronic hepatitis C
Antimicrobial Spectrum
Expected / intrinsic spectrum (EUCAST breakpoints & labels) — not local resistance. Source: openfda-label.
Viruses
| Organism | Activity | MIC |
|---|---|---|
| Hepatitis C | Active | — |
Class profile
| targetVirus | HCV (all genotypes) |
|---|---|
| viralClass | Flaviviridae (+ssRNA) |
| targetStep | NS5B RNA-dependent RNA polymerase (NUC inhibitor, chain terminator) |
| resistanceBarrier | Very high (S282T barely reduces susceptibility; clinically resistant variants rarely seen) |
| crossResistance | No cross-resistance to NS5A or NS3 inhibitors |
| source | DHHS/AASLD/manufacturer-PIL |
Contraindications
Source: Lexicomp
- Additional contraindications (not in US labeling): Hypersensitivity to sofosbuvir or any component of the formulation Absolute
- There are no contraindications listed in the manufacturer's labeling. When administered with ribavirin and peginterferon alfa, the contraindications to ribavirin and peginterferon alfa also apply. See Ribavirin and Peginterferon Alfa monographs Absolute
- males whose female partners may become pregnant Absolute
Adverse Reactions
Nervous system disorders (5)
Very Common chills · Fatigue · headache · insomnia · irritability
Hepatobiliary disorders (1)
Common Increased serum bilirubin
Renal and urinary disorders (1)
Common Increased creatine kinase
Blood and lymphatic system disorders (2)
Very Common Decreased hemoglobin
Common Thrombocytopenia
Gastrointestinal disorders (4)
Very Common decreased appetite · diarrhea · Nausea
Common Increased serum lipase
Skin and subcutaneous tissue disorders (2)
Very Common Pruritus · skin rash
Musculoskeletal and connective tissue disorders (2)
Very Common myalgia · Weakness
General disorders and administration site conditions (1)
Very Common Fever
Respiratory, thoracic and mediastinal disorders (1)
Very Common Flu-like symptoms
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Hepatitis B virus reactivation
Hepatitis B virus (HBV) reactivation has been reported in hepatitis C virus (HCV)/HBV co-infected patients who were receiving or had completed treatment with HCV direct-acting antivirals and were not receiving HBV antiviral therapy; some cases have resulted in fulminant hepatitis, hepatic failure, and death. Test all patients for evidence of current or prior HBV infection prior to initiation of sofosbuvir; monitor HCV/HBV co-infected patients for hepatitis flare or HBV reactivation during treatment and post-treatment follow-up. Initiate treatment for HBV infection as clinically indicated. HBV reactivation has been reported in HBsAg positive patients and in patients with serologic evidence of resolved HBV infection (ie, HBsAg negative and anti-HBc positive) and is characterized by an abrupt increase in HBV replication manifested as a rapid increase in serum HBV DNA level; reappearance of HBsAg may occur in patients with resolved HBV infection. Risk of HBV reactivation may be increased in patients receiving certain immunosuppressants or chemotherapeutic agents. Concurrent drug therapy issues:
Amiodarone
Symptomatic bradycardia (some requiring pacemaker intervention) has occurred in patients receiving amiodarone and a sofosbuvir-containing regimen. Fatal cardiac arrest occurred in a patient taking amiodarone and the ledipasvir/sofosbuvir combination product. Bradycardia generally occurred within hours to days following coadministration, however some cases have occurred 2 weeks following the initiation of sofosbuvir. The risk of bradycardia may be increased in patients taking beta blockers or patients with underlying cardiac comorbidities and/or advanced liver disease. Bradycardia generally resolves following discontinuation of HCV treatment. Coadministration of amiodarone and sofosbuvir in combination with another direct acting antiviral (DAA) is not recommended. However, if patients have no treatment alternatives, patients should have inpatient cardiac monitoring for the first 48 hours, followed by daily outpatient or self-monitoring of heart rate for at least the first 2 weeks of treatment. Due to the long half-life of amiodarone, cardiac monitoring (as described) is also recommended if amiodarone was discontinued just prior to beginning treatment with sofosbuvir. Patients should seek medical attention immediately if they experience fainting or near-fainting, dizziness, lightheadedness, malaise, weakness, excessive tiredness, shortness of breath, chest pains, confusion or memory problems.
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Hepatic impairment
Safety and efficacy have not been established in patients with decompensated cirrhosis. Other warnings/precautions:
Appropriate use
Do not use as monotherapy; use only as part of a multiple drug regimen for treatment of HCV; consult current HCV treatment guidelines for guidance (AASLD/IDSA 2016).
Pregnancy & Lactation
Pregnancy
Use in combination with ribavirin is contraindicated in pregnant women and males whose female partners are pregnant. Sofosbuvir is only to be used in combination with ribavirin or peginterferon alfa/ribavirin for the treatment of hepatitis C virus (HCV) (according to the manufacturer's labeling), and ribavirin use is contraindicated in pregnancy. If used in combination with ribavirin, all warnings related to the use of ribavirin and pregnancy and/or contraception should be followed. Mother-to-child transmission of HCV does not occur if the woman is not viremic, therefore, HCV-infected women of childbearing potential should postpone pregnancy until therapy is complete. Treatment of HCV is not recommended for women who are already pregnant (AASLD/IDSA 2016).
Lactation
It is not known if sofosbuvir is present in breast milk. According to the manufacturer, the decision to continue or discontinue breastfeeding during therapy should take into account the risk of infant exposure, the benefits of breastfeeding to the infant, and benefits of treatment to the mother. Breastfeeding is not linked to the spread of hepatitis C virus; however, if nipples are cracked or bleeding, breastfeeding is not recommended (CDC [Workowski 2015]). Mothers coinfected with HIV are dis
Monitoring
| Efficacy | Viral load (undetectable = success); CD4 count (HIV); hepatic enzymes and HBV/HCV DNA (hepatitis); clinical resolution of acute viral illness |
|---|---|
| Toxicity | Renal function (most antivirals are renally cleared); LFTs; resistance testing if virological failure; CBC |
| Clinical pearl | For HIV, undetectable viral load at 6 months predicts long-term treatment success. Resistance testing is mandatory at virological failure. |
| Counseling | Do not miss doses — even brief interruptions can cause viral rebound and resistance selection. Report any side effects early rather than stopping independently. |
Chemistry & Properties
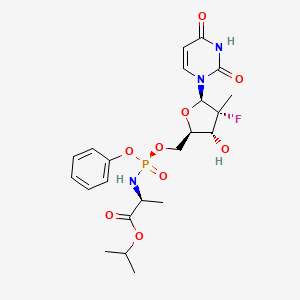
| Formula | C22H29FN3O9P |
|---|---|
| Molecular weight | 529.46 g/mol |
| IUPAC name | propan-2-yl (2S)-2-[[[(2R,3R,4R,5R)-5-(2,4-dioxopyrimidin-1-yl)-4-fluoro-3-hydroxy-4-methyloxolan-2-yl]methoxy-phenoxyphosphoryl]amino]propanoate |
| CAS | 1190307-88-0 |
| PubChem CID | 45375808 |
| InChIKey | TTZHDVOVKQGIBA-IQWMDFIBSA-N |
| logP | 1.66 (XLogP 1.0) |
| Polar surface area | 158.18 Ų |
| H-bond acceptors / donors | 10 / 3 |
| Drug-likeness (QED) | 0.31 |
| Lipinski violations | 1 |
SMILES
CC(C)OC(=O)[C@H](C)N[P@](=O)(OC[C@H]1O[C@@H](n2ccc(=O)[nH]c2=O)[C@](C)(F)[C@@H]1O)Oc1ccccc1Biology & Pharmacokinetics
Pharmacokinetics predicted
| Bioavailability | 10.0% |
|---|---|
| Half-life | 2.53 h |
| Volume of distribution | 0.621 L/kg |
| Protein binding | 67.7% |
| BBB penetrant | No |
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2C9 | Inhibitor | IC₅₀ 60.00000000000003 µM |
| CYP3A4 | Inhibitor | IC₅₀ 8.399999999999999 µM |
Transporters
BCRP (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MATE1 (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)OAT1 (Inhibitor)OAT3 (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)OCT1 (Inhibitor)OCT2 (Inhibitor)P-gp (Inhibitor)Transporter(unspecified) (Inhibitor)BCRP (Substrate)MATE1 (Substrate)MDR1 (Substrate)OAT1 (Substrate)OAT3 (Substrate)OATP1B1 (Substrate)OATP1B3 (Substrate)OCT1 (Substrate)OCT2 (Substrate)P-gp (Substrate)Transporter(unspecified) (Substrate)
Drug–drug interactions (8, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Apalutamide | major | |
| Enzalutamide | major | |
| Lorlatinib | major | |
| Dicoumarol | moderate | |
| Encorafenib | moderate | |
| Fostamatinib | moderate | |
| Warfarin | moderate | |
| Cyclosporine | minor |
Registered Products (3)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Grateziano | Tablet 400 mg | 28 tab | Modern Drug Store | 82.800 |
| Epclusa | Tablet 400 mg, 100 mg | 28 tab | Beta Drug Store | — |
| Harvoni 90mg /400mg | Tablet 400 mg, 90 mg | 28 tab | Beta Drug Store | — |