Azathioprine
Active form: Thioinosine Monophosphate.
JFDA label: Imuprin
- Malignancy:
Mechanism of Action
Inhibitor of Amidophosphoribosyltransferase — Amidophosphoribosyltransferase inhibitor; Inhibitor of DNA — DNA inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Amidophosphoribosyltransferase efficacy | INHIBITOR | PPAT |
| DNA efficacy | INHIBITOR |
Indications
Approved
- Renal transplantation
- Rheumatoid arthritis
Off-label
- Crohn disease
- Dermatomyositis/polymyositis
- Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome)
- Erythema multiforme
- Hepatitis (autoimmune)
- Immune thrombocytopenia, chronic (adults)
- Lupus nephritis (maintenance phase)
- Multiple sclerosis
- Pemphigus vulgaris
- Pericarditis, recurrent
- Psoriasis
- Ulcerative colitis (UC) (remission maintenance or reduction of steroid use)
- Uveitis (adults)
- Uveitis (children/adolescents)
Class profile
| mechanismClass | Antimetabolite (thiopurine prodrug of 6-MP, immunosuppressant/anticancer) |
|---|---|
| targetMolecule | HPRT + purine synthesis |
| targetPathway | Purine synthesis |
| generation | Prodrug |
| primaryTumors | ALL (historic),Immunosuppression/autoimmune |
| resistanceMechanisms | TPMT/NUDT15 rapid metabolizer,HPRT deletion |
| source | NCCN/OncoKB/Goodman&Gilman13ed |
Contraindications
Source: Lexicomp · Curated
- Hypersensitivity to azathioprine or any component of the formulation Absolute
- Previous hypersensitivity to mercaptopurine Absolute
- patients with rheumatoid arthritis and a history of treatment with alkylating agents (eg, cyclophosphamide, chlorambucil, melphalan) may have a prohibitive risk of malignancy with azathioprine treatment Absolute
- pregnancy (in patients with rheumatoid arthritis [see Pregnancy Considerations]) Absolute
Adverse Reactions
Nervous system disorders (1)
Not Known Malaise
Hepatobiliary disorders (4)
Not Known Hepatotoxicity · increased serum alkaline phosphatase · increased serum bilirubin · increased serum transaminases
Blood and lymphatic system disorders (3)
Not Known Leukopenia · neoplasia · thrombocytopenia
Gastrointestinal disorders (2)
Not Known diarrhea · Nausea and vomiting
Infections and infestations (1)
Not Known Increased susceptibility to infection (renal transplant 20%; rheumatoid arthritis Neuromuscular & skeletal: Myalgia
General disorders and administration site conditions (1)
Not Known Fever
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Gastrointestinal toxicity
The frequency of gastrointestinal adverse effects (nausea and vomiting) may be decreased with dividing dose or administering after meals. Gastrointestinal hypersensitivity with severe nausea and vomiting has been reported; diarrhea, rash, fever, malaise, myalgia, hypotension, and liver enzyme abnormalities may also occur. Symptoms usually develop within the first several weeks of treatment and are generally reversible upon discontinuation; may recur upon rechallenge.
Hematologic toxicity
Dose-related hematologic toxicities (leukopenia, thrombocytopenia, and anemias, including macrocytic anemia and/or pancytopenia) may occur; may be severe and/or delayed. Thiopurine methyltransferase (TPMT) genotyping or phenotyping may help to identify patients who are at an increased risk for developing azathioprine toxicity. Patients with intermediate TPMT activity may be at increased risk for hematologic toxicity at conventional azathioprine doses; patients with low or absent TPMT activity are at risk for severe, life-threatening myelotoxicity. Myelosuppression may be more severe with renal transplants undergoing rejection. Monitor CBC with differential and platelets weekly during the first month, then twice a month for 2 months, then monthly (or more frequently if clinically indicated). May require treatment interruption or dose reduction. Leukopenia does not correlate with therapeutic effect and the dose should not be increased intentionally to lower the white blood cell count.
Hepatotoxicity
Hepatotoxicity (transaminase, bilirubin, and/or alkaline phosphatase elevations) may occur, usually in renal transplant patients. Usually occurs within 6 months of transplant and is normally reversible with discontinuation. Monitor liver function periodically. Rarely, hepatic sinusoidal obstruction syndrome (SOS; formerly called veno-occlusive disease [VOD]) has been reported; discontinue if hepatic SOS is suspected.
Infections
Chronic immunosuppression increases the risk of serious, sometimes fatal, infections (bacterial, viral, fungal, protozoal, and opportunistic), including reactivation of latent infections.
Malignancy
Chronic immunosuppression with azathioprine (a purine antimetabolite), increases the risk of malignancy. Malignancies reported have included post-transplant lymphoma and hepatosplenic T-cell lymphoma (HSTCL) in patients with inflammatory bowel disease. Health care providers using this medication should be very familiar with this risk, as well as with the mutagenic potential to both men and women, and with possible hematologic toxicities. Patients should be informed of the risk for malignancy development. HSTCL is a rare white blood cell cancer that is usually fatal and has predominantly occurred in adolescents and young adults treated for Crohn disease or ulcerative colitis and receiving TNF blockers (eg, adalimumab, certolizumab pegol, etanercept, golimumab), azathioprine, and/or mercaptopurine. Most cases of HSTCL have occurred in patients treated with a combination of immunosuppressant agents, although there have been reports of HSTCL in patients receiving azathioprine or mercaptopurine monotherapy. Renal transplant patients are known to be at increased risk for malignancy (eg, skin cancer, lymphoma), the risk is increased with aggressive immunosuppression. Limit sun and ultraviolet light exposure and use appropriate sun protection.
Progressive multifocal leukoencephalopathy
Cases of JC virus-associated infection resulting in progressive multifocal leukoencephalopathy (PML), have been reported in patients treated with immunosuppressants, including azathioprine (some cases have been fatal). Risk factors for PML include treatment with immunosuppressants and immune system impairment. Consider a diagnosis of PML in any patient presenting with new-onset neurological manifestations; consultation with a neurologist as clinically indicated may be warranted. Consider decreasing the degree of immunosuppression with respect to the risk of organ rejection in transplant patients. Disease-related concerns:
Hepatic impairment
Use with caution in patients with hepatic impairment.
Renal impairment
Use with caution in patients with renal impairment; dosage reductions may be necessary.
TPMT deficiency
Patients with genetic deficiency of TPMT are more sensitive to myelosuppressive effects. Patients with intermediate TPMT activity may be at risk for increased myelosuppression; those with low or absent TPMT activity are at risk for developing severe and life-threatening hematologic toxicity. TPMT genotyping or phenotyping may assist in identifying patients at risk for developing toxicity. Consider TPMT testing in patients with abnormally low CBC unresponsive to dose reduction. TPMT testing does not substitute for CBC monitoring. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
Mercaptopurine
Azathioprine is metabolized to mercaptopurine; concomitant use may result in profound myelosuppression and should be avoided.
TPMT or xanthine oxidase inhibitors
Patients on concurrent therapy with drugs which may inhibit TPMT (eg, olsalazine) or xanthine oxidase (eg, allopurinol) may be sensitive to myelosuppressive effects. Dose adjustment of azathioprine may be recommended when used concurrently with allopurinol; patients with low or absent TPMT activity may require further dose reductions or discontinuation.
Vaccines
Immune response to vaccines may be diminished. Other warnings/precautions:
Experienced health care provider
Should be prescribed by health care providers familiar with the risks, including hematologic toxicities and mutagenic potential.
Pregnancy & Lactation
Pregnancy
Caution
Acceptable alternative to mycophenolate (which is teratogenic) in transplant patients. TPMT testing before use reduces bone marrow toxicity. Lowest effective dose
Lactation
Azathioprine is excreted in breast milk. Due to potential for serious adverse reactions in the nursing infant, breastfeeding is not recommended by the manufacturer. Although there are theoretical concerns of adverse events in nursing infants, available guidelines do not recommend mothers be discouraged from breastfeeding during therapy (Durst 2015; Flint 2016)
Monitoring
| Efficacy | Tumour response (RECIST criteria, tumour markers, imaging); progression-free survival; performance status (ECOG/Karnofsky) |
|---|---|
| Toxicity | CBC with differential (nadir timing depends on agent); LFTs; renal function; ECG (QT for relevant agents); echocardiogram for cardiotoxic agents (anthracyclines, trastuzumab); cumulative dose tracking for dose-limited toxicities |
| Clinical pearl | Treatment response is assessed after 2–3 cycles. Grade 3–4 toxicities typically require dose reduction or interruption per protocol-defined criteria. |
| Counseling | Attend all scheduled blood tests and imaging appointments. Report fever > 38°C (risk of neutropaenic sepsis — medical emergency), unusual bleeding, or new pain immediately. |
Chemistry & Properties
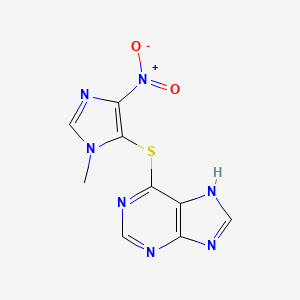
| Formula | C9H7N7O2S |
|---|---|
| Molecular weight | 277.27 g/mol |
| IUPAC name | 6-(3-methyl-5-nitroimidazol-4-yl)sulfanyl-7H-purine |
| CAS | 446-86-6 |
| PubChem CID | 2265 |
| InChIKey | LMEKQMALGUDUQG-UHFFFAOYSA-N |
| logP | 1.15 (XLogP 0.1) |
| Polar surface area | 115.42 Ų |
| H-bond acceptors / donors | 8 / 1 |
| Drug-likeness (QED) | 0.43 |
| Lipinski violations | 0 |
SMILES
Cn1cnc([N+](=O)[O-])c1Sc1ncnc2[nH]cnc12Biology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2C9 | Substrate | — |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)OAT1 (Inhibitor)OAT3 (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)OATP2B1 (Inhibitor)OCT1 (Inhibitor)P-gp (Inhibitor)MDR1 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Adalimumab | major | |
| Allopurinol | major | |
| Bacillus calmette-guerin substrain tice live antigen | major | |
| Baricitinib | major | |
| Certolizumab pegol | major | |
| Cladribine | major | |
| Clozapine | major | |
| Deferiprone | major | |
| Etanercept | major | |
| Febuxostat | major | |
| Fingolimod | major | |
| Golimumab | major | |
| Infliximab | major | |
| Leflunomide | major | |
| Measles virus vaccine live attenuated | major | |
| Mercaptopurine | major | |
| Mumps virus strain B level jeryl lynn live antigen | major | |
| Natalizumab | major | |
| Ozanimod | major | |
| Ribavirin | major | |
| Rotavirus vaccine | major | |
| Rubella virus vaccine | major | |
| Samarium (153Sm) lexidronam | major | |
| Siponimod | major | |
| Smallpox (Vaccinia) Vaccine, Live | major | |
| Talimogene laherparepvec | major | |
| Teriflunomide | major | |
| Tofacitinib | major | |
| Typhoid vaccine (live) | major | |
| Upadacitinib | major | |
| Varicella Zoster Vaccine (Recombinant) | major | |
| Yellow Fever Vaccine | major | |
| Abatacept | moderate | |
| Abemaciclib | moderate | |
| Acalabrutinib | moderate | |
| Aflibercept | moderate | |
| Aldesleukin | moderate | |
| Alefacept | moderate | |
| Alemtuzumab | moderate | |
| Altretamine | moderate |
Showing 40 of 100+.
Registered Products (5)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Imuprin | Tablet 50 mg | 20 tab pack varies | JAWEDA INT. DRUD STORE | 3.530 |
| Azamun 50mg F.c tab | Film-Coated Tablet 50 mg | 100 tab | Reda Jardaneh Drug Store | 10.510 |
| Imuprin | Tablet 50 mg | 100 tab pack varies | JAWEDA INT. DRUD STORE | 16.320 |
| Imuran Tablet | Tablet 50 mg | 100 tab | Suleiman Tannous & Sons Co. Ltd | 19.660 |
| Imuprin | Tablet 50 mg | 1000 tab pack varies | JAWEDA INT. DRUD STORE | 132.480 |