Sitagliptin
JFDA label: Januvia Tablet
Mechanism of Action
Sitagliptin inhibits dipeptidyl peptidase IV (DPP-IV) enzyme resulting in prolonged active incretin levels. Incretin hormones (eg, glucagon-like peptide-1 [GLP-1] and glucose-dependent insulinotropic polypeptide [GIP]) regulate glucose homeostasis by increasing insulin synthesis and release from pancreatic beta cells and decreasing glucagon secretion from pancreatic alpha cells. Decreased glucagon secretion results in decreased hepatic glucose production. Under normal physiologic circumstances, incretin hormones are released by the intestine throughout the day and levels are increased in response to a meal; incretin hormones are rapidly inactivated by the DPP-IV enzyme.
Indications
Approved
- Diabetes mellitus, type 2
Class profile
| mechanismClass | DPP-4 inhibitor (incretin enhancer) |
|---|---|
| insulinSecretagogue | 0 |
| weightEffect | Neutral |
| hypoglycemiaRisk | None |
| renalContraindicated | 0 |
| cardioProtective | 0 |
| renalProtective | 0 |
| source | ADA-EASD2023/Maruthur2016 |
Contraindications
Source: Lexicomp · Curated
- Serious hypersensitivity (eg, anaphylaxis, angioedema) to sitagliptin or any component of the formulation Absolute
- Type 1 diabetes mellitus Absolute
Adverse Reactions
Nervous system disorders (1)
Common Headache
Renal and urinary disorders (1)
Not Known Increased serum creatinine
Immune system disorders (1)
Rare Angioedema (class effect)
Metabolism and nutrition disorders (1)
Common Hypoglycemia
Gastrointestinal disorders (3)
Rare Pancreatitis (class concern)
Not Known Diarrhea · nausea
Musculoskeletal and connective tissue disorders (1)
Uncommon Severe arthralgia
Infections and infestations (1)
Common Nasopharyngitis / upper respiratory tract infection
Respiratory, thoracic and mediastinal disorders (1)
Common Nasopharyngitis
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Arthralgia
Severe and disabling arthralgia has been reported with DPP-IV inhibitor use; onset may occur within one day to years after treatment initiation and may resolve with discontinuation of therapy. Some patients may experience a recurrence of symptoms if DPP-IV inhibitor therapy resumed.
Bullous pemphigoid
DPP-4 inhibitor use has been associated with development of bullous pemphigoid; cases have typically resolved with topical or systemic immunosuppressive therapy and discontinuation of DPP-4 inhibitor therapy. Advise patients to report development of blisters or erosions. Discontinue therapy if bullous pemphigoid is suspected and consider referral to a dermatologist.
Hypersensitivity reactions
Serious hypersensitivity reactions, including anaphylaxis, angioedema, and exfoliative skin reactions, such as Stevens-Johnson syndrome, have been reported; discontinue if signs/symptoms of hypersensitivity reactions occur. Events have generally been noted within the first 3 months of therapy, and may occur with the initial dose. Use with caution if patient has experienced angioedema with other dipeptidyl peptidase IV (DPP-IV) inhibitor use.
Pancreatitis
Cases of acute pancreatitis (including hemorrhagic and necrotizing with some fatalities) have been reported with use. Monitor for signs/symptoms of pancreatitis; discontinue use immediately if pancreatitis is suspected and initiate appropriate management. Use with caution in patients with a history of pancreatitis as it is not known if this population is at greater risk.
Renal effects
Worsening renal function, including acute renal failure, sometimes requiring dialysis has been reported. Disease-related concerns:
Cardiovascular disease
In cardiovascular outcome trials of patients with type 2 diabetes and atherosclerotic cardiovascular disease, treatment with other DPP-4 inhibitors has been associated with heart failure. Use sitagliptin with caution in patients at risk for heart failure (eg, history of heart failure or renal impairment) and monitor for signs and symptoms of heart failure during therapy; consider discontinuation if heart failure develops. In a scientific statement from the American Heart Association, sitagliptin has been determined to be an agent that may exacerbate underlying myocardial dysfunction (magnitude: major) (AHA [Page 2016]). However, in one large randomized, double-blinded trial in patients with type 2 diabetes and established cardiovascular disease (history of major CAD, ischemic cerebrovascular disease, or atherosclerotic peripheral arterial disease), the occurrence of the primary composite cardiovascular outcome (cardiovascular death, nonfatal MI, nonfatal stroke, or hospitalization for unstable angina) with sitagliptin was found to be noninferior to placebo. In addition, the rate of hospitalization for heart failure did not differ between the two groups (Green 2015; McGuire 2016).
Renal impairment
Use with caution in patients with moderate to severe renal dysfunction and end-stage renal disease (ESRD) requiring hemodialysis or peritoneal dialysis; dosing adjustment required. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Other warnings/precautions:
Appropriate use
Not indicated for use in patients with insulin-dependent diabetes mellitus (IDDM) (type 1) or in patients with diabetic ketoacidosis (DKA).
Patient education
Diabetes self-management education is essential to maximize the effectiveness of therapy.
Pregnancy & Lactation
Pregnancy
Adverse events have not been observed in animal reproduction studies. In women with diabetes, maternal hyperglycemia can be associated with congenital malformations as well as adverse effects in the fetus, neonate, and the mother (ACOG 2005; ADA 2018c; Kitzmiller 2008; Metzger 2007). To prevent adverse outcomes, prior to conception and throughout pregnancy, maternal blood glucose and HbA1c should be kept as close to target goals as possible but without causing significant hypoglycemia (ACOG 2013; ADA 2018c; Blumer 2013; Kitzmiller 2008). Agents other than sitagliptin are currently recommended to treat diabetes in pregnant women (ADA 2018c). Health care providers are encouraged to enroll women exposed to sitagliptin during pregnancy in the registry (1-800-986-8999).
Lactation
It is not known if sitagliptin is present in breast milk. According to the manufacturer, the decision to continue or discontinue breastfeeding during therapy should take into account the risk of infant exposure, the benefits of breastfeeding to the infant, and benefits of treatment to the mother.
Monitoring
| Efficacy | HbA1c every 3 months initially, then every 6–12 months when stable; fasting and post-prandial blood glucose; patient-reported hypoglycaemia episodes |
|---|---|
| Toxicity | Hypoglycaemia symptoms; eGFR for renally-cleared agents; weight; blood pressure |
| Clinical pearl | Individualise HbA1c targets based on patient age, comorbidities, and hypoglycaemia risk. Targets of < 7% are appropriate for most patients but < 8% may be safer in frail elderly. |
| Counseling | Monitor blood glucose regularly. Know how to recognise and treat hypoglycaemia. Keep carbohydrate snacks available. |
Chemistry & Properties
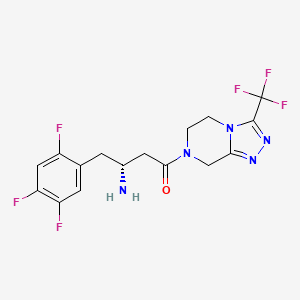
| Formula | C16H15F6N5O |
|---|---|
| Molecular weight | 407.32 g/mol |
| IUPAC name | (3R)-3-amino-1-[3-(trifluoromethyl)-6,8-dihydro-5H-[1,2,4]triazolo[4,3-a]pyrazin-7-yl]-4-(2,4,5-trifluorophenyl)butan-1-one |
| CAS | 486460-32-6 |
| PubChem CID | 4369359 |
| InChIKey | MFFMDFFZMYYVKS-SECBINFHSA-N |
| logP | 2.02 (XLogP 0.7) |
| Polar surface area | 77.04 Ų |
| H-bond acceptors / donors | 5 / 1 |
| Drug-likeness (QED) | 0.62 |
| Lipinski violations | 0 |
SMILES
N[C@@H](CC(=O)N1CCn2c(nnc2C(F)(F)F)C1)Cc1cc(F)c(F)cc1FBiology & Pharmacokinetics
Pharmacokinetics predicted
| Bioavailability | 10.0% |
|---|---|
| Half-life | 0.715 h |
| Volume of distribution | 3.844 L/kg |
| Protein binding | 58.0% |
| BBB penetrant | No |
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2C19 | Substrate | — |
| CYP3A4 | Substrate | — |
Receptor binding (top 1)
| Target | Action | Affinity |
|---|---|---|
| dipeptidyl peptidase 4 (DPP4) | Inhibitor | pIC50 8.1 |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OCT(unspecified) (Inhibitor)OCT1 (Inhibitor)OCT2 (Inhibitor)P-gp (Inhibitor)Transporter(unspecified) (Inhibitor)MDR1 (Substrate)MRP2 (Substrate)OAT (Substrate)OAT1 (Substrate)OAT3 (Substrate)OATP4C1 (Substrate)OCT(unspecified) (Substrate)OCT1 (Substrate)OCT2 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Bexarotene | major | |
| Gatifloxacin | major | |
| Acetazolamide | moderate | |
| Acetohexamide | moderate | |
| Alimemazine | moderate | |
| Aloe Vera Leaf | moderate | |
| Alpelisib | moderate | |
| Amprenavir | moderate | |
| Apalutamide | moderate | |
| Aripiprazole | moderate | |
| Asenapine | moderate | |
| Asparaginase Erwinia chrysanthemi | moderate | |
| Asparaginase Escherichia coli | moderate | |
| Atazanavir | moderate | |
| Benazepril | moderate | |
| Bendroflumethiazide | moderate | |
| Benzphetamine | moderate | |
| Benzthiazide | moderate | |
| Betamethasone | moderate | |
| Bortezomib | moderate | |
| Brentuximab vedotin | moderate | |
| Brexpiprazole | moderate | |
| Brigatinib | moderate | |
| Bumetanide | moderate | |
| Cabozantinib | moderate | |
| Calaspargase pegol | moderate | |
| Captopril | moderate | |
| Cariprazine | moderate | |
| Ceritinib | moderate | |
| Chlorothiazide | moderate | |
| Chlorpromazine | moderate | |
| Chlorpropamide | moderate | |
| Chlorthalidone | moderate | |
| Chromic chloride | moderate | |
| Chromium picolinate | moderate | |
| Cinoxacin | moderate | |
| Ciprofloxacin | moderate | |
| Clarithromycin | moderate | |
| Clozapine | moderate | |
| Conjugated estrogens | moderate |
Showing 40 of 100+.
Registered Products (20)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| SITAPRIL 50 | Tablet 64.25 mg | 30 tab | Reda Jardaneh Drug Store | 4.580 |
| SITAPRIL 100 | Tablet 128.50 mg | 30 tab | Reda Jardaneh Drug Store | 7.500 |
| Sitamac | Tablet 100 mg | 28 tab | Sun Set Drug Store | 8.670 |
| Januqan | Tablet 50 mg | 30 tab | Itqan Pharmaceutical Industries | 12.230 |
| Reglu | Tablet Sitagliptin 50 mg | 30 tab | AL-TAQADDOM PHARMACEUTICAL INDUSTRIES/JORDAN | 14.410 |
| Sitaglin | Tablet 50 mg | 30 tab | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN | 14.410 |
| Sitago-met | Tablet 1000 mg, equivalent to 50 mg Sitagliptin Base | 60 tab | SANA PHARMACEUTICAL INDUSTRY/JORDAN | 14.420 |
| SITAMET 50/1000 Tablet | Tablet 1000 mg, 50 mg | 60 tab | Al-Motakadema Pharmaceutical LTD | 15.170 |
| JUVESTA 100 mg Film coated tablets | Film-Coated Tablet 128.5 mg | 30 tab | Masrouji drug store | 16.330 |
| jeneptin | Tablet Metformin Hcl 1000 mg, Sitagliptin phosphate monohydrate 64.25 mg | 60 tab | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN / General | 18.500 |
| Xitavia-M 50/1000 mg F.C Tablet | Film-Coated Tablet 10000 mg, 60 mg | 60 tab | SAVVY PHARMA/JORDAN | 19.500 |
| Janumet | Tablet 500 mg, (as Sitagliptin Phosphate)50 mg | 56 tab | Adatco Drug Store | 20.020 |
| Janumet | Tablet 1000 mg, (as Sitagliptin Phosphate)50 mg | 56 tab | Adatco Drug Store | 20.020 |
| Januqan | Tablet 100 mg | 30 tab | Itqan Pharmaceutical Industries | 20.050 |
| Reglu | Tablet Sitagliptin 100 mg | 30 tab | AL-TAQADDOM PHARMACEUTICAL INDUSTRIES/JORDAN | 23.630 |
| Sitaglin | Tablet 100 mg | 30 tab | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN | 23.630 |
| Xitavia | Tablet 100 mg | 30 tab | Savvy Pharma | 23.630 |
| Januvia Tablet | Tablet 100 mg | 28 tab | Adatco Drug Store | 24.510 |
| Steglujan | Tablet 100 mg, 15 mg | 30 tab | Adatco Drug Store | 52.640 |
| Steglujan | Tablet 100 mg, 5 mg | 30 tab | Adatco Drug Store | 52.640 |