Erdafitinib
JFDA label: Balversa
Mechanism of Action
Inhibitor of Fibroblast growth factor receptor — Fibroblast growth factor receptor inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Fibroblast growth factor receptor efficacy | INHIBITOR |
Indications
Approved
- Carcinoma, Transitional Cell — urothelial carcinoma
- Neoplasms — neoplasm
- Urinary Bladder Neoplasms — urothelial carcinoma
Off-label
- Carcinoma, Non-Small-Cell Lung
- Carcinoma, Squamous Cell
- Multiple Myeloma
- Prostatic Neoplasms
- Prostatic Neoplasms, Castration-Resistant
Contraindications
Source: openFDA
- None. None. ( 4 ) Absolute
Adverse Reactions
Cardiac disorders (1)
Common Including Acute Myocardial Infarction
Vascular disorders (1)
Very Common And Peripheral Edema
Hepatobiliary disorders (2)
Common And Increased Alanine Aminotransferase · Increased Aspartate Aminotransferase
Renal and urinary disorders (4)
Common Acute Kidney Injury · And Acute Kidney Injury · Hematuria
Uncommon Renal Failure
Metabolism and nutrition disorders (1)
Common Hyponatremia
Gastrointestinal disorders (5)
Very Common Diarrhea · Of Patients Who Received Balversa Included Nausea · Stomatitis · Vomiting
Common Dry Mouth
Skin and subcutaneous tissue disorders (3)
Very Common Actions For Dose Reductions Included Nail Disorders · Nail Disorders
Common Of Patients Included Nail Disorders
Musculoskeletal and connective tissue disorders (1)
Very Common And Arthralgia
Eye disorders (6)
Very Common Eye Disorders
Common And Blurred Vision · And Eye Disorders · Central Serous Retinopathy · Discontinuation Included Central Serous Retinopathy · S Adverse Reactions Were Central Serous Retinopathy
Infections and infestations (3)
Common Of Patients Included Urinary Tract Infection · Pneumonia · Urinary Tract Infection
General disorders and administration site conditions (13)
Very Common Extremity Pain · Of Patients Who Received Balversa Included Pyrexia · Palmar-Plantar Erythrodysesthesia Syndrome · Pyrexia · Ring Dosage Interruption Included Hyperphosphatemia
Common And Fatigue · And General Physical Health Deterioration · And Hyperphosphatemia · Fatigue · General Physical Health Deterioration · Hyperphosphatemia · Including Sudden Death · Palmar-Plantar Erythro-Dysesthesia Syndrome
Respiratory, thoracic and mediastinal disorders (2)
Very Common Epistaxis
Uncommon And Cardiorespiratory Arrest
Dosing
Source: openFDA
Warnings & Precautions
Source: openFDA
Warnings & Precautions
Ocular disorders: BALVERSA can cause central serous retinopathy/retinal pigment epithelial detachment (CSR/RPED). Perform monthly ophthalmological examinations during the first four months of treatment, every 3 months afterwards, and at any time for visual symptoms. Withhold BALVERSA when CSR/RPED occurs and permanently discontinue if it does not resolve within 4 weeks or if Grade 4 in severity. ( 2.3 , 5.1 ) Hyperphosphatemia: Increases in phosphate levels are a pharmacodynamic effect of BALVERSA. Monitor for hyperphosphatemia and manage with dose modifications when required. ( 2.3 , 5.2 ) Embryo-fetal toxicity: Can cause fetal harm. Advise patients of the potential risk to the fetus and to use effective contraception ( 5.3 , 8.1 , 8.3)
Ocular Disorders BALVERSA can cause ocular disorders, including centra
Ocular Disorders BALVERSA can cause ocular disorders, including central serous retinopathy/retinal pigment epithelial detachment (CSR/RPED) resulting in visual field defect. In the pooled safety population [see Adverse Reactions (6) ] , CSR/RPED occurred in 22% of patients treated with BALVERSA, with a median time to first onset of 46 days. In 104 patients with CSR, 40% required dose interruptions and 56% required dose reductions; 2.9% of BALVERSA-treated patients required permanent discontinuation for CSR. Of the 24 patients who restarted BALVERSA after dose interruption with or without dose reduction, 67% had recurrence and/or worsening of CSR after restarting. CSR was ongoing in 41% of the 104 patients at the time of last evaluation. Dry eye symptoms occurred in 26% of BALVERSA-treated patients. All patients should receive dry eye prophylaxis with ocular demulcents as needed. Perform monthly ophthalmological examinations during the first 4 months of treatment and every 3 months afterwards, and urgently at any time for visual symptoms. Ophthalmological examination should include assessment of visual acuity, slit lamp examination, fundoscopy, and optical coherence tomography. Withhold or permanently discontinue BALVERSA based on severity and/or ophthalmology exam findings [see Dosage and Administration (2.3) ] .
Hyperphosphatemia and Soft Tissue Mineralization BALVERSA can cause hy
Hyperphosphatemia and Soft Tissue Mineralization BALVERSA can cause hyperphosphatemia leading to soft tissue mineralization, cutaneous calcinosis, non-uremic calciphylaxis and vascular calcification. Increases in phosphate levels are a pharmacodynamic effect of BALVERSA [see Pharmacodynamics (12.2) ]. In the pooled safety population [see Adverse Reactions (6) ], increased phosphate occurred in 73% of BALVERSA-treated patients. The median onset time of increased phosphate was 16 days (range: 8–421) after initiating BALVERSA. Twenty-four percent of patients received phosphate binders during treatment with BALVERSA. Vascular calcification was observed in 0.2% of patients treated with BALVERSA. Monitor for hyperphosphatemia throughout treatment. Restrict dietary phosphate intake (600–800 mg daily) and avoid concomitant use of agents that may increase serum phosphate levels. If serum phosphate is above 7.0 mg/dL, consider adding an oral phosphate binder until serum phosphate level returns to <7.0 mg/dL. Withhold, dose reduce, or permanently discontinue BALVERSA based on duration and severity of hyperphosphatemia according to Table 2 [see Dosage and Administration (2.3) ].
Embryo-Fetal Toxicity Based on the mechanism of action and findings in
Embryo-Fetal Toxicity Based on the mechanism of action and findings in animal reproduction studies, BALVERSA can cause fetal harm when administered to a pregnant woman. In an embryo-fetal toxicity study, oral administration of erdafitinib to pregnant rats during the period of organogenesis caused malformations and embryo-fetal death at maternal exposures that were less than the human exposures at the maximum human recommended dose based on area under the curve (AUC). Advise pregnant women of the potential risk to the fetus. Advise female patients of reproductive potential to use effective contraception during treatment with BALVERSA and for one month after the last dose. Advise male patients with female partners of reproductive potential to use effective contraception during treatment with BALVERSA and for one month after the last dose [see Use in Specific Populations (8.1 , 8.3) and Clinical Pharmacology (12.1) ] .
Pregnancy & Lactation
Lactation
The manufacturer recommends that breastfeeding be discontinued during erdafitinib therapy and for 1 month after the final dose.
Chemistry & Properties
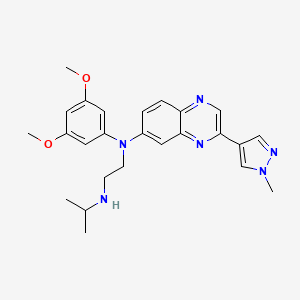
| Formula | C25H30N6O2 |
|---|---|
| Molecular weight | 446.56 g/mol |
| IUPAC name | N'-(3,5-dimethoxyphenyl)-N'-[3-(1-methylpyrazol-4-yl)quinoxalin-6-yl]-N-propan-2-ylethane-1,2-diamine |
| CAS | 1346242-81-6 |
| PubChem CID | 67462786 |
| InChIKey | OLAHOMJCDNXHFI-UHFFFAOYSA-N |
| logP | 4.18 (XLogP 3.2) |
| Polar surface area | 77.33 Ų |
| H-bond acceptors / donors | 8 / 1 |
| Drug-likeness (QED) | 0.41 |
| Lipinski violations | 0 |
SMILES
COc1cc(OC)cc(N(CCNC(C)C)c2ccc3ncc(-c4cnn(C)c4)nc3c2)c1Biology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP1A2 | Inhibitor | — |
| CYP1A2 | Substrate | — |
| CYP2C19 | Inhibitor | — |
| CYP2C19 | Substrate | — |
| CYP2C8 | Inhibitor | — |
| CYP2C9 | Substrate | — |
| CYP2D6 | Inhibitor | — |
| CYP2D6 | Substrate | — |
| CYP3A4 | Inhibitor | — |
Receptor binding (top 5)
| Target | Action | Affinity |
|---|---|---|
| fibroblast growth factor receptor 1 (FGFR1) | Inhibitor | pIC50 8.9 |
| fibroblast growth factor receptor 2 (FGFR2) | Inhibitor | pIC50 8.6 |
| fibroblast growth factor receptor 3 (FGFR3) | Inhibitor | pIC50 8.5 |
| fibroblast growth factor receptor 4 (FGFR4) | Inhibitor | pIC50 8.2 |
| kinase insert domain receptor (KDR) | Inhibitor | pIC50 7.4 |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OCT2 (Inhibitor)P-gp (Inhibitor)MDR1 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Aluminum hydroxide | major | |
| Apalutamide | major | |
| Calcifediol | major | |
| Calcipotriol (topical) | major | |
| Calcitriol | major | |
| Calcium Phosphate | major | |
| Calcium acetate | major | |
| Calcium carbonate | major | |
| Calcium citrate | major | |
| Ceritinib | major | |
| Cholecalciferol | major | |
| Clarithromycin | major | |
| Cobicistat | major | |
| Dabrafenib | major | |
| Dexamethasone | major | |
| Dihydrotachysterol | major | |
| Doxercalciferol | major | |
| Enzalutamide | major | |
| Ergocalciferol | major | |
| Iron sucrose | major | |
| Ketoconazole | major | |
| Lanthanum carbonate | major | |
| Lorlatinib | major | |
| Lumacaftor | major | |
| Magaldrate | major | |
| Magnesium carbonate | major | |
| Magnesium chloride | major | |
| Magnesium citrate | major | |
| Magnesium gluconate | major | |
| Magnesium hydroxide | major | |
| Magnesium oxide | major | |
| Magnesium sulfate | major | |
| Mitotane | major | |
| Paricalcitol | major | |
| Sevelamer | major | |
| Sodium glycerophosphate | major | |
| Tetraferric tricitrate decahydrate | major | |
| Abemaciclib | moderate | |
| Afatinib | moderate | |
| Apixaban | moderate |
Showing 40 of 100+.
Registered Products (6)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Balversa | Tablet 3 mg | 56 tab pack varies | Adatco Drug Store | — |
| Balversa | Tablet 5 mg | 28 tab | Adatco Drug Store | — |
| Balversa | Tablet 4 mg | 28 tab pack varies | Adatco Drug Store | — |
| Balversa | Tablet 4 mg | 14 tab pack varies | Adatco Drug Store | — |
| Balversa | Tablet 4 mg | 56 tab pack varies | Adatco Drug Store | — |
| Balversa | Tablet 3 mg | 84 tab pack varies | Adatco Drug Store | — |