Pemetrexed
JFDA label: Pemitra 500mg
Mechanism of Action
Inhibitor of Dihydrofolate reductase — Dihydrofolate reductase inhibitor; Inhibitor of Thymidylate synthase — Thymidylate synthase inhibitor; Inhibitor of Trifunctional purine biosynthetic protein adenosine-3 — GAR transformylase inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Dihydrofolate reductase efficacy | INHIBITOR | DHFR |
| Thymidylate synthase efficacy | INHIBITOR | TYMS |
| Trifunctional purine biosynthetic protein adenosine-3 efficacy | INHIBITOR | GART |
Indications
Approved
- Mesothelioma
- Non-small cell lung cancer (NSCLC), nonsquamous
Off-label
- Bladder cancer, metastatic
- Cervical cancer, persistent or recurrent
- Malignant pleural mesothelioma (single agent and off-label combination)
- Ovarian cancer, platinum-resistant
- Thymic malignancies, metastatic
Class profile
| mechanismClass | Antimetabolite (multi-targeted antifolate) |
|---|---|
| targetMolecule | DHFR + TS + GARFT (folate cycle) |
| targetPathway | Folate/pyrimidine/purine synthesis |
| generation | Multi-targeted antifolate |
| primaryTumors | Non-squamous NSCLC,Mesothelioma |
| resistanceMechanisms | TS overexpression,Reduced polyglutamation (FPGS),Methylenetetrahydrofolate reductase (MTHFR) status |
| source | NCCN/OncoKB/Goodman&Gilman13ed |
Contraindications
Source: Lexicomp
- Additional contraindications (not in the US labeling): Concomitant yellow fever vaccine Absolute
- Severe hypersensitivity to pemetrexed or any component of the formulation Absolute
Adverse Reactions
Cardiac disorders (1)
Common Edema
Nervous system disorders (2)
Very Common Fatigue
Common Neuropathy
Blood and lymphatic system disorders (2)
Very Common Anemia · neutropenia
Immune system disorders (1)
Common Hypersensitivity reaction, increased lacrimation
Gastrointestinal disorders (8)
Very Common anorexia · diarrhea · Nausea · stomatitis · vomiting
Common abdominal pain, febrile neutropenia, increased serum AST · constipation · Mucositis
Skin and subcutaneous tissue disorders (5)
Very Common Desquamation · skin rash
Common alopecia · erythema multiforme · Pruritus
Respiratory, thoracic and mediastinal disorders (1)
Very Common Pharyngitis
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Bone marrow suppression
Pemetrexed may cause severe myelosuppression, including anemia, neutropenia, thrombocytopenia and/or pancytopenia; frequent laboratory monitoring is necessary (myelosuppression is often dose-limiting). Severe myelosuppression may require blood transfusion. Prophylactic folic acid and vitamin B12 supplements are necessary to reduce hematologic toxicity, febrile neutropenia and infection; initiate supplementation 1 week before the first dose of pemetrexed and continue for 21 days after the last pemetrexed dose (the risk for myelosuppression is higher in patients who did not receive vitamin supplementation). Monitor blood counts at the beginning of each cycle, and as clinically indicated. Dose reductions in subsequent cycles may be required due to myelosuppression.
Cutaneous reactions
Serious and occasionally fatal dermatologic toxicity may occur; pretreatment with dexamethasone is necessary to reduce the incidence and severity of cutaneous reactions. Rarely, Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported. Permanently discontinue pemetrexed for severe and life-threatening bullous, blistering, or exfoliating dermatologic toxicity.
Gastrointestinal toxicity
Gastrointestinal toxicity may occur; prophylactic folic acid and vitamin B12 supplements are necessary to reduce gastrointestinal toxicity. Initiate supplementation 1 week before the first dose of pemetrexed and continue for 21 days after the last pemetrexed dose.
Hypersensitivity
Hypersensitivity (including allergic reaction) has been reported with pemetrexed.
Nephrotoxicity
Pemetrexed may cause severe (and potentially fatal) renal toxicity (renal toxicity may occur with single-agent pemetrexed or when used in combination with other chemotherapy agents). Measure creatinine clearance prior to each dose and monitor renal function throughout treatment. May require therapy discontinuation. Withhold pemetrexed treatment for creatinine clearance • Pulmonary toxicity: Interstitial pneumonitis has been observed with use; may be serious and/or fatal. Interrupt therapy and evaluate promptly for acute onset new or progressive pulmonary symptoms (eg, dyspnea, cough, or fever). If interstitial pneumonitis is confirmed, permanently discontinue pemetrexed.
Radiation recall
Radiation recall may occur in patients administered pemetrexed who received radiation previously (weeks to years). Monitor for inflammation or blistering in areas of prior radiation treatment; permanently discontinue pemetrexed if radiation recall is confirmed. Disease-related concerns:
Renal impairment
Pemetrexed is primarily cleared by the kidneys; decreased renal function results in increased toxicity. The manufacturer does not recommend use if CrCl • Third space fluid: Although the effect of third space fluid on pemetrexed pharmacokinetics has not been fully defined, studies have determined pemetrexed concentrations in patients with mild-to-moderate ascites/pleural effusions were similar to concentrations in trials of patients without third space fluid accumulation. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
Ibuprofen
Ibuprofen may reduce the clearance of pemetrexed. In patients with CrCl 45 to 79 mL/minute, interrupt ibuprofen therapy 2 days prior to, during, and 2 days after pemetrexed therapy. If concomitant use cannot be avoided, monitor for myelosuppression, renal, and gastrointestinal toxicity.
Pregnancy & Lactation
Pregnancy
Adverse effects were observed in animal reproduction studies. Based on the mechanism of action, pemetrexed may cause fetal harm if administered to a pregnant woman. Women of reproductive potential should use effective contraception during treatment and for at least 6 months after the last pemetrexed dose. Males with female partners of reproductive potential should use effective contraception during treatment and for 3 months after the last pemetrexed dose. Pemetrexed may impair fertility in males.
Lactation
It is not known if pemetrexed is present in breast milk. Due to the potential for serious adverse reactions in the breastfed infant, breastfeeding is not recommended during treatment and for 1 week after the final dose.
Monitoring
| Efficacy | Tumour response (RECIST criteria, tumour markers, imaging); progression-free survival; performance status (ECOG/Karnofsky) |
|---|---|
| Toxicity | CBC with differential (nadir timing depends on agent); LFTs; renal function; ECG (QT for relevant agents); echocardiogram for cardiotoxic agents (anthracyclines, trastuzumab); cumulative dose tracking for dose-limited toxicities |
| Clinical pearl | Treatment response is assessed after 2–3 cycles. Grade 3–4 toxicities typically require dose reduction or interruption per protocol-defined criteria. |
| Counseling | Attend all scheduled blood tests and imaging appointments. Report fever > 38°C (risk of neutropaenic sepsis — medical emergency), unusual bleeding, or new pain immediately. |
Chemistry & Properties
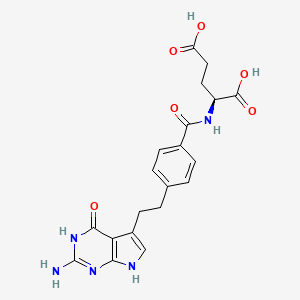
| Formula | C20H21N5O6 |
|---|---|
| Molecular weight | 427.42 g/mol |
| IUPAC name | (2S)-2-[[4-[2-(2-amino-4-oxo-3,7-dihydropyrrolo[2,3-d]pyrimidin-5-yl)ethyl]benzoyl]amino]pentanedioic acid |
| CAS | 137281-23-3 |
| PubChem CID | 135410875 |
| InChIKey | WBXPDJSOTKVWSJ-ZDUSSCGKSA-N |
| logP | 0.67 (XLogP 0.2) |
| Polar surface area | 191.26 Ų |
| H-bond acceptors / donors | 6 / 6 |
| Drug-likeness (QED) | 0.29 |
| Lipinski violations | 1 |
SMILES
Nc1nc2[nH]cc(CCc3ccc(C(=O)N[C@@H](CCC(=O)O)C(=O)O)cc3)c2c(=O)[nH]1Biology & Pharmacokinetics
Pharmacokinetics predicted
| Bioavailability | 10.0% |
|---|---|
| Half-life | 1.87 h |
| Volume of distribution | 0.174 L/kg |
| Protein binding | 78.2% |
| BBB penetrant | No |
Receptor binding (top 2)
| Target | Action | Affinity |
|---|---|---|
| Dihyrofolate Reductase, DHFR | Binding | pKi 5.2 |
| Thymidylate Synthase | Binding | pKi 5.0 |
Transporters
BCRP (Inhibitor)BSEP (Inhibitor)MRP1 (Inhibitor)MRP5 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)OAT3 (Substrate)OATP2B1 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Adalimumab | major | |
| Bacillus calmette-guerin substrain tice live antigen | major | |
| Baricitinib | major | |
| Certolizumab pegol | major | |
| Cladribine | major | |
| Clozapine | major | |
| Deferiprone | major | |
| Etanercept | major | |
| Fingolimod | major | |
| Golimumab | major | |
| Infliximab | major | |
| Leflunomide | major | |
| Measles virus vaccine live attenuated | major | |
| Mumps virus strain B level jeryl lynn live antigen | major | |
| Natalizumab | major | |
| Ozanimod | major | |
| Rotavirus vaccine | major | |
| Rubella virus vaccine | major | |
| Samarium (153Sm) lexidronam | major | |
| Siponimod | major | |
| Smallpox (Vaccinia) Vaccine, Live | major | |
| Talimogene laherparepvec | major | |
| Teriflunomide | major | |
| Thalidomide | major | |
| Tofacitinib | major | |
| Typhoid vaccine (live) | major | |
| Upadacitinib | major | |
| Varicella Zoster Vaccine (Recombinant) | major | |
| Yellow Fever Vaccine | major | |
| Acetylsalicylic acid | moderate | |
| Acyclovir | moderate | |
| Aldesleukin | moderate | |
| Alefacept | moderate | |
| Alemtuzumab | moderate | |
| Allopurinol | moderate | |
| Amikacin | moderate | |
| Amikacin (liposome) | moderate | |
| Aminosalicylic acid | moderate | |
| Amoxicillin | moderate | |
| Amphotericin B | moderate |
Showing 40 of 100+.
Registered Products (7)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Alimta | Vial 500 mg | 1 vial | THE ARAB DRUG STORE P.S.C | — |
| Pemetrexed EVER Pharma | Vial 25 mg mg/1 ml | 1 vial pack varies | Sabbagh Drug Store | — |
| Pemetrexed EVER Pharma | Vial 25 mg mg/1 ml | 1 vial pack varies | Sabbagh Drug Store | — |
| Pemitra | Vial 500 mg | 1 vial | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Pemitra 100mg Powder For Concentrate For Solution For Infusion Vials | Infusion 100 mg | 1 vial | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Pexate | Vial 500 mg | 1 vial | شركة مستودع ادوية جرينلاند | — |
| Trixem 500mg/vial powder for solution for infusion | Infusion 500 mg | 1 vial | MS PHARMA/JORDAN | — |