Enalapril
Active form: Enalaprilat Anhydrous.
🧬 Cross-allergy: ACE inhibitors
JFDA label: Lapril Tablets
- Fetal toxicity:
Mechanism of Action
Competitive inhibitor of angiotensin-converting enzyme (ACE); prevents conversion of angiotensin I to angiotensin II, a potent vasoconstrictor; results in lower levels of angiotensin II which causes an increase in plasma renin activity and a reduction in aldosterone secretion
Indications
Approved
- Asymptomatic left ventricular dysfunction
- Coronary artery disease (CAD) and hypertension
- Diabetes and hypertension
- HF
- Hypertension
Off-label
- Aldosteronism (diagnosis)
- Bartter's syndrome
- Hypertension secondary to scleroderma renal crisis
- Hypertensive crisis
- Idiopathic edema
- Non–ST-elevation acute coronary syndrome
- Postmyocardial infarction for prevention of ventricular failure
Contraindications
Source: Lexicomp · Curated
- Additional contraindications (not in US labeling): Concomitant use with aliskiren-containing drugs in patients with moderate-to-severe renal impairment (GFR 2) Absolute
- History of ACE-inhibitor-associated angioedema Absolute
- Hypersensitivity to enalapril or any component of the formulation Absolute
- Pregnancy — second and third trimester Absolute
- angioedema related to previous treatment with an ACE inhibitor Absolute
- coadministration with or within 36 hours of switching to or from a neprilysin inhibitor (eg, sacubitril). Documentation of allergenic cross-reactivity for ACE inhibitors is limited. However, because of similarities in chemical structure and/or pharmacologic actions, the possibility of cross-sensitivity cannot be ruled out with certainty Absolute
- concomitant use with aliskiren in patients with diabetes mellitus Absolute
- idiopathic or hereditary angioedema Absolute
Adverse Reactions
Cardiac disorders (5)
Common chest pain · Hypotension · orthostatic effect · orthostatic hypotension · syncope
Vascular disorders (1)
Common Hypotension (first dose)
Nervous system disorders (5)
Common Dizziness · Dizziness · fatigue · Headache · headache
Renal and urinary disorders (1)
Common Renal insufficiency (in patients with bilateral renal artery stenosis or hypovolemia)
Immune system disorders (1)
Rare Angioedema
Metabolism and nutrition disorders (1)
Uncommon Hyperkalaemia
Gastrointestinal disorders (7)
Common Abdominal pain · anorexia · constipation · diarrhea · dysgeusia · nausea · vomiting
Skin and subcutaneous tissue disorders (2)
Common Skin rash
Uncommon Rash
Musculoskeletal and connective tissue disorders (1)
Common Weakness
Investigations (1)
Common Elevated serum creatinine
General disorders and administration site conditions (1)
Common Fatigue
Respiratory, thoracic and mediastinal disorders (4)
Very Common Dry cough
Common Bronchitis · cough · dyspnea
Other (3)
Very Common Renal: Increased serum creatinine
Not Known Frequency ranges include data from hypertension and heart failure trials. Higher rates of adverse reactions have generally been noted in patients with CHF. However · the frequency of adverse effects associated with placebo is also increased in this population
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Angioedema
At any time during treatment (especially following first dose) angioedema may occur rarely with ACE inhibitors; it may involve the head and neck (potentially compromising airway) or the intestine (presenting with abdominal pain). African-Americans may be at an increased risk. Risk may also be increased with concomitant use of mTOR inhibitor (eg, everolimus) therapy or a neprilysin inhibitor (eg, sacubitril). Prolonged frequent monitoring may be required especially if tongue, glottis, or larynx are involved as they are associated with airway obstruction. Patients with a history of airway surgery may have a higher risk of airway obstruction. Aggressive early and appropriate management is critical. Use in patients with idiopathic or hereditary angioedema or previous angioedema associated with ACE inhibitor therapy is contraindicated.
Cholestatic jaundice
A rare toxicity associated with ACE inhibitors includes cholestatic jaundice, which may progress to fulminant hepatic necrosis (some fatal); discontinue if marked elevation of hepatic transaminases or jaundice occurs.
Cough
An ACE inhibitor cough is a dry, hacking, nonproductive one that usually occurs within the first few months of treatment and should generally resolve within 1 to 4 weeks after discontinuation of the ACE inhibitor. Other causes of cough should be considered (eg, pulmonary congestion in patients with HF) and excluded prior to discontinuation.
Hematologic effects
Another ACE inhibitor, captopril, has been associated with neutropenia with myeloid hypoplasia and agranulocytosis; anemia and thrombocytopenia have also occurred. Patients with renal impairment are at high risk of developing neutropenia. Patients with both renal impairment and collagen vascular disease (eg, systemic lupus erythematosus) are at an even higher risk of developing neutropenia. Periodically monitor CBC with differential in these patients.
Hyperkalemia
May occur with ACE inhibitors; risk factors include renal dysfunction, diabetes mellitus, concomitant use of potassium-sparing diuretics, potassium supplements, and/or potassium-containing salts. Use cautiously, if at all, with these agents and monitor potassium closely.
Hypersensitivity reactions
Anaphylactic/anaphylactoid reactions can occur with ACE inhibitors. Severe anaphylactoid reactions may be seen during hemodialysis (eg, CVVHD) with high-flux dialysis membranes (eg, AN69), and rarely, during low density lipoprotein apheresis with dextran sulfate cellulose. Rare cases of anaphylactoid reactions have been reported in patients undergoing sensitization treatment with hymenoptera (bee, wasp) venom while receiving ACE inhibitors.
Hypotension/syncope
Symptomatic hypotension with or without syncope can occur with ACE inhibitors (usually with the first several doses). Effects are most often observed in volume-depleted patients; correct volume depletion prior to initiation. Close monitoring of patient is required, especially with initial dosing and dosing increases; blood pressure must be lowered at a rate appropriate for the patient's clinical condition. Although dose reduction may be necessary, hypotension is not a reason for discontinuation of future ACE inhibitor use, especially in patients with HF where a reduction in systolic blood pressure is a desirable observation.
Renal function deterioration
May be associated with deterioration of renal function and/or increases in serum creatinine, particularly in patients with low renal blood flow (eg, renal artery stenosis, HF) whose GFR is dependent on efferent arteriolar vasoconstriction by angiotensin II; deterioration may result in oliguria, acute renal failure, and progressive azotemia. Small increases in serum creatinine may occur following initiation; consider discontinuation only in patients with progressive and/or significant deterioration in renal function (Bakris 2000). Disease-related concerns:
Aortic stenosis
Use with caution in patients with severe aortic stenosis; may reduce coronary perfusion resulting in ischemia.
Cardiovascular disease
Initiation of therapy in patients with ischemic heart disease or cerebrovascular disease warrants close observation due to the potential consequences posed by falling blood pressure (eg, MI, stroke). Fluid replacement, if needed, may restore blood pressure; therapy may then be resumed. Discontinue therapy in patients whose hypotension recurs.
Collagen vascular disease
Use with caution in patients with collagen vascular disease especially with concomitant renal impairment; may be at increased risk for hematologic toxicity.
Hypertrophic cardiomyopathy (HCM) with outflow tract obstruction
Use with caution in patients with HCM and outflow tract obstruction since reduction in afterload may worsen symptoms associated with this condition (ACCF/AHA [Gersh 2011]).
Renal artery stenosis
Use with caution in patients with unstented unilateral/bilateral renal artery stenosis. When unstented bilateral renal artery stenosis is present, use is generally avoided due to the elevated risk of deterioration in renal function unless possible benefits outweigh risks.
Renal impairment
Use with caution in preexisting renal insufficiency; dosage adjustment may be needed. Avoid rapid dosage escalation which may lead to further renal impairment. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Black patients
ACE inhibitors effectiveness is less in black patients than in non-blacks. In addition, ACE inhibitors cause a higher rate of angioedema in black than in non-black patients.
Pregnancy
Drugs that act on the renin-angiotensin system can cause injury and death to the developing fetus. Discontinue as soon as possible once pregnancy is detected.
Surgical patients
In patients on chronic ACE inhibitor therapy, intraoperative hypotension may occur with induction and maintenance of general anesthesia; use with caution before, during, or immediately after major surgery. Cardiopulmonary bypass, intraoperative blood loss, or vasodilating anesthesia increases endogenous renin release. Use of ACE inhibitors perioperatively will blunt angiotensin II formation and may result in hypotension. However, discontinuation of therapy prior to surgery is controversial. If continued preoperatively, avoidance of hypotensive agents during surgery is prudent (Hillis 2011). Based on current research and clinical guidelines in patients undergoing non-cardiac surgery, continuing ACE inhibitors is reasonable in the perioperative period. If ACE inhibitors are held before surgery, it is reasonable to restart postoperatively as soon as clinically feasible (ACC/AHA [Fleisher 2014]). Dosage forms specific issues:
Oral solution
May contain sodium benzoate/benzoic acid; benzoic acid (benzoate) is a metabolite of benzyl alcohol. Large amounts of benzyl alcohol (≥99 mg/kg/day) have been associated with a potentially fatal toxicity ("gasping syndrome") in neonates; the "gasping syndrome" consists of metabolic acidosis, respiratory distress, gasping respirations, CNS dysfunction (including convulsions, intracranial hemorrhage), hypotension, and cardiovascular collapse (AAP 1997; CDC 1982). Some data suggest that benzoate displaces bilirubin from protein-binding sites (Ahlfors 2001); avoid or use dosage forms containing benzyl alcohol derivative with caution in neonates. See manufacturer’s labeling.
Pregnancy & Lactation
Pregnancy
Avoid
Contraindicated in T2/T3. Switch to methyldopa, labetalol, or nifedipine for hypertension. If inadvertently used in T1, perform serial ultrasound for amniotic fluid and fetal anatomy
Lactation
Enalapril and enalaprilat are present in breast milk. Due to the potential for serious adverse reactions in the breastfed infant, the manufacturer recommends a decision be made whether to discontinue breastfeeding or to discontinue the drug, taking into account the importance of treatment to the mother. Some guidelines consider enalapril to be acceptable for use in breastfeeding women. Monitoring of the breastfed child's weight for the first 4 weeks is recommended (Regitz-Zagrosek 2011).
Monitoring
| Clinical pearl | Blood pressure; serum creatinine and potassium; if patient has collagen vascular disease and/or renal impairment, periodically monitor CBC with differential 2013 ACCF/AHA Heart Failure guideline recommendations: Within 1-2 weeks after initiation and periodically thereafter, reassess renal function and serum potassium especially in patients with preexisting hypotension, hyponatremia, diabetes mellitus, azotemia, or those taking potassium supplements (ACCF/AHA [Yancy 2013]). |
|---|
Chemistry & Properties
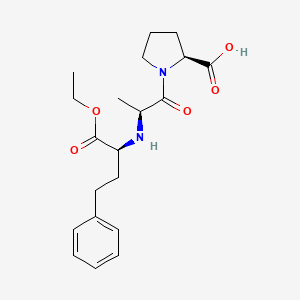
| Formula | C20H28N2O5 |
|---|---|
| Molecular weight | 376.45 g/mol |
| IUPAC name | (2S)-1-[(2S)-2-[[(2S)-1-ethoxy-1-oxo-4-phenylbutan-2-yl]amino]propanoyl]pyrrolidine-2-carboxylic acid |
| CAS | 75847-73-3 |
| PubChem CID | 5388962 |
| InChIKey | GBXSMTUPTTWBMN-XIRDDKMYSA-N |
| logP | 1.6 (XLogP -0.1) |
| Polar surface area | 95.94 Ų |
| H-bond acceptors / donors | 5 / 2 |
| Drug-likeness (QED) | 0.64 |
| Lipinski violations | 0 |
SMILES
CCOC(=O)[C@H](CCc1ccccc1)N[C@@H](C)C(=O)N1CCC[C@H]1C(=O)OBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP3A4 | Substrate | — |
Transporters
ASBT (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MATE1 (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)NTCP (Inhibitor)OAT1 (Inhibitor)OAT2 (Inhibitor)OAT3 (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)OATP2B1 (Inhibitor)OCT1 (Inhibitor)OCTN1 (Inhibitor)OCTN2 (Inhibitor)P-gp (Inhibitor)PEPT1 (Inhibitor)MRP2 (Substrate)OATP1A2 (Substrate)OATP1B1 (Substrate)P-gp (Substrate)PEPT1 (Substrate)PEPT2 (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Leflunomide | major | |
| Potassium Iodide | major | |
| Potassium acetate | major | |
| Potassium bicarbonate | major | |
| Potassium chloride | major | |
| Potassium citrate | major | |
| Potassium gluconate | major | |
| Teriflunomide | major | |
| Acetohexamide | moderate | |
| Acetylsalicylic acid | moderate | |
| Aldesleukin | moderate | |
| Alimemazine | moderate | |
| Alogliptin | moderate | |
| Alteplase | moderate | |
| Amifostine | moderate | |
| Anistreplase | moderate | |
| Asparaginase Escherichia coli | moderate | |
| Azathioprine | moderate | |
| Betamethasone | moderate | |
| Brentuximab vedotin | moderate | |
| Brimonidine (ophthalmic) | moderate | |
| Brimonidine (topical) | moderate | |
| Bromotheophylline | moderate | |
| Budesonide | moderate | |
| Bupropion | moderate | |
| Canagliflozin | moderate | |
| Celecoxib | moderate | |
| Chlorpropamide | moderate | |
| Clofarabine | moderate | |
| Codeine | moderate | |
| Corticotropin | moderate | |
| Cyclosporine | moderate | |
| Dalteparin | moderate | |
| Dapagliflozin | moderate | |
| Deflazacort | moderate | |
| Desmopressin | moderate | |
| Dexamethasone | moderate | |
| Diclofenac | moderate | |
| Diphenhydramine | moderate | |
| Doxepin | moderate |
Showing 40 of 100+.
Registered Products (32)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Lapril Tablets | Tablet 5 mg | 20 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 2.330 |
| Lapril Tablets | Tablet 10 mg | 20 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 3.330 |
| ACE press 5 Tablet | Tablet 5 mg | 30 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 3.500 |
| Lapril Tablets | Tablet 5 mg | 30 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 3.500 |
| Korandil | Tablet Enalapril Maleate 5 mg | 30 tab | JAWEDA INT. DRUD STORE | 3.890 |
| Angiotec | Tablet 5 mg | 30 tab | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 4.540 |
| Korandil | Tablet Enalapril Maleate 10 mg | 30 tab | JAWEDA INT. DRUD STORE | 4.720 |
| ACE press tablet | Tablet 10 mg | 30 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 5.000 |
| Lapril Tablets | Tablet 10 mg | 30 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 5.000 |
| Lapril Tablets | Tablet 20 mg | 20 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 5.030 |
| Angiotec | Tablet 10 mg | 30 tab pack varies | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 6.190 |
| Angiotec | Tablet 20 mg | 20 tab pack varies | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 6.260 |
| Vasopril | Tablet 10 mg | 30 tab | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN | 6.900 |
| Lapril Tablets | Tablet 20 mg | 30 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 7.540 |
| ACE press tablet | Tablet 20 mg | 30 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 8.500 |
| Korandil | Tablet Enalapril Maleate 20 mg | 30 tab | JAWEDA INT. DRUD STORE | 8.880 |
| Angiozide tablet | Tablet 12.5 mg, 20 mg | 20 tab | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 9.000 |
| Vasopril | Tablet 20 mg | 30 tab pack varies | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN | 9.000 |
| Eneas | Tablet 10 mg, 20 mg | 30 tab | Ibn Rushd Drug Store | 16.760 |
| Angiotec | Tablet 20 mg | 100 tab pack varies | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 28.800 |
| ACE press 5 TAB | Tablet 5 mg | 500 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 50.750 |
| ACE press 5 TAB | Tablet 5 mg | 510 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 51.000 |
| ACE press tablet | Tablet 10 mg | 500 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 72.500 |
| ACE press tablet | Tablet 10 mg | 510 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 73.950 |
| Lapril Tablets | Tablet 5 mg | 1000 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 93.340 |
| ACE press tablet | Tablet 20 mg | 500 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 123.250 |
| ACE press tablet | Tablet 20 mg | 510 tab pack varies | Jordan Sweden Medical & Sterilization Co. | 123.250 |
| Lapril Tablets | Tablet 10 mg | 1000 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 133.330 |
| Angiotec | Tablet 10 mg | 1005 tab pack varies | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 176.000 |
| Lapril tablets | Tablet 20 mg | 1000 tab pack varies | MIDDLE EAST PHARMA&CHEMICAL IND/JORDAN | 213.630 |
| Angiotec | Tablet 20 mg | 1000 tab pack varies | THE JORDANIAN PHARMACEUTICAL MANUFACTURING COMPANY/JORDAN | 266.050 |
| Vasopril Tablet | Tablet 20 mg | 1000 tab pack varies | AL-RAM PHARMA.INDUS.CO.LTD/JORDAN | 348.310 |