Dasatinib
JFDA label: Elpida
Mechanism of Action
Inhibitor of Bcr/Abl fusion protein — Bcr/Abl fusion protein inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Bcr/Abl fusion protein efficacy | INHIBITOR |
Indications
Approved
- Acute lymphoblastic leukemia
- Adults
- Chronic myeloid leukemia
- Pediatrics
Off-label
- Gastrointestinal stromal tumor (GIST)
Class profile
| mechanismClass | Tyrosine kinase inhibitor (TKI) |
|---|---|
| targetMolecule | BCR-ABL,SRC kinases |
| targetPathway | BCR-ABL/SRC signaling |
| generation | 2nd generation ABL TKI |
| primaryTumors | CML,Ph+ ALL |
| resistanceMechanisms | T315I mutation (primary resistance),T315A mutation (dasatinib-specific) |
| source | NCCN/OncoKB/Goodman&Gilman13ed |
Contraindications
Source: Lexicomp
- Hypersensitivity to dasatinib or any other component of the formulation Absolute
- There are no contraindications listed in the manufacturer's US labeling Absolute
- breast-feeding Absolute
Adverse Reactions
Cardiac disorders (2)
Very Common Facial edema · peripheral edema
Nervous system disorders (12)
Very Common fatigue · Headache · pain
Common chills · depression · dizziness · drowsiness · insomnia · Intracranial hemorrhage · myasthenia · neuropathy · peripheral neuropathy
Hepatobiliary disorders (4)
Common ascites · increased serum ALT · increased serum AST · Increased serum bilirubin
Renal and urinary disorders (1)
Common Increased serum creatinine
Blood and lymphatic system disorders (6)
Very Common anemia · febrile neutropenia · hemorrhage · neutropenia · Thrombocytopenia
Common Bruise
Metabolism and nutrition disorders (5)
Very Common Fluid retention
Common Growth suppression · hyperuricemia · weight gain · weight loss
Gastrointestinal disorders (15)
Very Common abdominal pain · Diarrhea · nausea · vomiting
Common abdominal distention · change in appetite · colitis (including neutropenic colitis) · Constipation · dysgeusia · dyspepsia · enterocolitis · gastritis · gastrointestinal hemorrhage · mucositis · stomatitis
Skin and subcutaneous tissue disorders (9)
Very Common pruritus · Skin rash
Common Acne vulgaris · alopecia · dermatitis · eczema · hyperhidrosis · urticaria · xeroderma
Musculoskeletal and connective tissue disorders (5)
Very Common Musculoskeletal pain, dyspnea
Common abnormal bone growth (children; epiphyses delayed fusion) · Muscle spasm · stiffness · weakness
Eye disorders (4)
Common Blurred vision · decreased visual acuity · dry eye syndrome · visual disturbance
Ear and labyrinth disorders (1)
Common Tinnitus
Infections and infestations (3)
Very Common Infection
Common Herpes virus infection · sepsis
General disorders and administration site conditions (3)
Very Common Fever · Localized edema
Common Soft tissue injury (oral)
Other (12)
Common cardiac arrhythmia · Cardiac conduction disturbance · cardiac disease · chest pain · edema · flushing · hypertension · ischemic heart disease · palpitations · pericardial effusion · prolonged Q-T interval on ECG · tachycardia
Respiratory, thoracic and mediastinal disorders (7)
Common cough · pneumonia · pneumonitis · pulmonary edema · Pulmonary hypertension · pulmonary infiltrates · upper respiratory tract infection
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Bone marrow suppression
Severe dose-related bone marrow suppression (thrombocytopenia, neutropenia, anemia) is associated with dasatinib treatment. Hematologic toxicity is usually reversible with dosage adjustment and/or temporary treatment interruption. The incidence of myelosuppression is higher in patients with advanced chronic myeloid leukemia (CML) and Ph+ acute lymphoblastic leukemia (ALL). Monitor blood counts every 2 weeks for 12 weeks and then every 3 months thereafter or as clinically indicated (for chronic phase CML) or weekly for the first 2 months, then monthly thereafter or as clinically necessary (for accelerated or blast phase CML or for ALL).
Cardiovascular adverse events
Dasatinib may cause cardiac dysfunction; cardiac ischemic events, cardiac fluid retention-related events, and conduction abnormalities (arrhythmia and palpitations) have been reported. Monitor for signs and symptoms of cardiac dysfunction. Monitor blood pressure routinely during dasatinib treatment; if indicated, initiate appropriate antihypertensive treatment to reduce the risk for cardiotoxicity (Armenian 2017).
Dermatologic toxicity
Cases of severe mucocutaneous dermatologic reactions (including Stevens-Johnson syndrome and erythema multiforme) have been reported with dasatinib. Discontinue dasatinib if severe mucocutaneous reaction occurs and other etiologies have been ruled out.
Fluid retention
Dasatinib may cause fluid retention, including pleural and pericardial effusions, pulmonary hypertension, and generalized or superficial edema. A prompt chest x-ray (or other appropriate diagnostic imaging) is recommended for symptoms suggestive of effusion (new or worsening dyspnea on exertion or at rest, pleuritic chest pain, or dry cough). Fluid retention may be managed with supportive care (diuretics or corticosteroids); thoracentesis and oxygen therapy may be necessary for severe fluid retention; consider dose reduction or treatment interruption. Utilizing once-daily dosing is associated with a decreased frequency of fluid retention. The risk for pleural effusion is increased in patients with hypertension, prior cardiac history and a twice a day administration schedule; interrupt treatment for grade ≥2 effusion; may consider reinitiating at a reduced dose after resolution (Quintás-Cardama 2007). Grade 3 or 4 fluid retention/pleural effusion was observed in adults and grade 1 or 2 fluid retention was observed in pediatric patients. Use with caution in patients where fluid accumulation may be poorly tolerated, such as in cardiovascular disease (HF or hypertension) and pulmonary disease.
Hemorrhage
Dasatinib may cause serious and fatal bleeding, including grades 3 and higher CNS hemorrhage. The most frequent hemorrhage site was gastrointestinal. Grades 3 or 4 hemorrhage usually required treatment interruptions and transfusions. Most bleeding events in clinical studies were associated with severe thrombocytopenia, although dasatinib may also cause platelet dysfunction. Concomitant medications that inhibit platelet function or anticoagulants may increase the risk of bleeding.
Pulmonary arterial hypertension
Dasatinib may increase the risk for pulmonary arterial hypertension (PAH) in both adult and pediatric patients. PAH may occur at any time after starting treatment, including after >12 months of therapy. Evaluate for underlying cardiopulmonary disease prior to therapy initiation and during therapy; evaluate and rule out alternative etiologies in patients with symptoms suggestive of PAH (eg, dyspnea, fatigue, hypoxia, fluid retention) and interrupt therapy if symptoms are severe. Discontinue permanently with confirmed PAH diagnosis (may be reversible upon discontinuation).
QT prolongation
Dasatinib may increase the risk for QT interval prolongation; there are reports of patients with QTcF >500 msec. Use caution in patients at risk for QT prolongation, including patients with long QT syndrome, patients taking antiarrhythmic medications or other medications that lead to QT prolongation or potassium-wasting diuretics, patients with cumulative high-dose anthracycline therapy, and conditions which cause hypokalemia or hypomagnesemia. Correct hypokalemia and hypomagnesemia prior to and during dasatinib therapy.
Tumor lysis syndrome
Tumor lysis syndrome (TLS) has been reported in patients with resistance to imatinib therapy, usually in patients with advanced phase disease. Risk for TLS is higher in patients with advanced stage disease and/or a high tumor burden; monitor patients at risk more frequently. Maintain adequate hydration and correct uric acid levels prior to treatment; monitor electrolyte levels. Disease-related concerns:
Hepatic impairment
Use with caution in patients with hepatic impairment due to extensive hepatic metabolism. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Use with caution in patients taking anticoagulants or medications interfering with platelet function; not studied in clinical trials. Avoid concomitant use with CYP3A4 inducers and inhibitors; if concomitant use cannot be avoided, consider dasatinib dosage adjustments.
Drugs that affect gastric pH
Elevated gastric pH may reduce dasatinib bioavailability; do not administer proton pump inhibitors and H2 blockers concomitantly with dasatinib. If needed, may consider antacid administration separated by at least 2 hours before or 2 hours after the dasatinib dose. Special populations:
Elderly
Patients 65 years of age and older are more likely to experience toxicity (compared with younger patients).
Pediatrics
Adverse reactions associated with bone growth and development have been reported in pediatric studies of chronic phase CML (including a report of severe [grade 3] growth retardation). Cases have included epiphyses delayed fusion, osteopenia, growth retardation, and gynecomastia; some cases resolved during treatment. Monitor bone growth/development in pediatric patients.
Pregnancy & Lactation
Pregnancy
Dasatinib crosses the placenta, with fetal plasma and amniotic concentrations comparable to maternal concentrations. Adverse effects, including hydrops fetalis and fetal leukopenia and thrombocytopenia have been reported following maternal exposure to dasatinib. Women of reproductive potential should use effective contraception during treatment and for 30 days after the final dasatinib dose. Pregnant women are advised to avoid exposure to crushed or broken tablets.
Lactation
It is not known if dasatinib is present in breast milk. Due to the potential for serious adverse reactions in the breastfed infant, breastfeeding is not recommended by the manufacturer during treatment and for 2 weeks following the final dose.
Monitoring
| Efficacy | Tumour response (RECIST criteria, tumour markers, imaging); progression-free survival; performance status (ECOG/Karnofsky) |
|---|---|
| Toxicity | CBC with differential (nadir timing depends on agent); LFTs; renal function; ECG (QT for relevant agents); echocardiogram for cardiotoxic agents (anthracyclines, trastuzumab); cumulative dose tracking for dose-limited toxicities |
| Clinical pearl | Treatment response is assessed after 2–3 cycles. Grade 3–4 toxicities typically require dose reduction or interruption per protocol-defined criteria. |
| Counseling | Attend all scheduled blood tests and imaging appointments. Report fever > 38°C (risk of neutropaenic sepsis — medical emergency), unusual bleeding, or new pain immediately. |
Chemistry & Properties
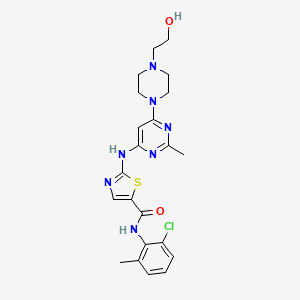
| Formula | C22H28ClN7O3S |
|---|---|
| Molecular weight | 506.03 g/mol |
| IUPAC name | N-(2-chloro-6-methylphenyl)-2-[[6-[4-(2-hydroxyethyl)piperazin-1-yl]-2-methylpyrimidin-4-yl]amino]-1,3-thiazole-5-carboxamide |
| CAS | 302962-49-8 |
| PubChem CID | 3062316 |
| InChIKey | XHXFZZNHDVTMLI-UHFFFAOYSA-N |
| logP | 3.31 (XLogP 3.6) |
| Polar surface area | 106.51 Ų |
| H-bond acceptors / donors | 9 / 3 |
| Drug-likeness (QED) | 0.47 |
| Lipinski violations | 0 |
SMILES
Cc1nc(Nc2ncc(C(=O)Nc3c(C)cccc3Cl)s2)cc(N2CCN(CCO)CC2)n1.OBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP1A2 | Substrate | — |
| CYP2C19 | Substrate | — |
| CYP2C9 | Inhibitor | IC₅₀ 49.99999999999999 µM |
| CYP2C9 | Substrate | — |
| CYP3A4 | Inhibitor | Ki 6.3 µM |
| CYP3A4 | Substrate | — |
Receptor binding (top 6)
| Target | Action | Affinity |
|---|---|---|
| ABL proto-oncogene 1, non-receptor tyrosine kinase (ABL1) | Inhibitor | pKd 10.5 |
| ABL proto-oncogene 1, non-receptor tyrosine kinase (ABL1) | Inhibitor | pIC50 9.6 |
| SRC proto-oncogene, non-receptor tyrosine kinase (SRC) | Inhibitor | pIC50 9.1 |
| salt inducible kinase 1 (SIK1) | Inhibitor | pIC50 8.5 |
| salt inducible kinase 2 (SIK2) | Inhibitor | pIC50 8.5 |
| SIK family kinase 3 (SIK3) | Inhibitor | pIC50 8.0 |
Transporters
BCRP (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)ENT2 (Inhibitor)MATE1 (Inhibitor)MATE2 (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP2B1 (Inhibitor)OCT1 (Inhibitor)OCT2 (Inhibitor)OCT3 (Inhibitor)P-gp (Inhibitor)BCRP (Substrate)MDR1 (Substrate)MRP4 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Abciximab | major | |
| Acalabrutinib | major | |
| Acetylsalicylic acid | major | |
| Adalimumab | major | |
| Alteplase | major | |
| Amiodarone | major | |
| Amisulpride | major | |
| Amprenavir | major | |
| Anagrelide | major | |
| Anisindione | major | |
| Anistreplase | major | |
| Antithrombin III human | major | |
| Apalutamide | major | |
| Apixaban | major | |
| Ardeparin | major | |
| Argatroban | major | |
| Arsenic trioxide | major | |
| Atazanavir | major | |
| Avapritinib | major | |
| Bacillus calmette-guerin substrain tice live antigen | major | |
| Baricitinib | major | |
| Bedaquiline | major | |
| Bepridil | major | |
| Betrixaban | major | |
| Binimetinib | major | |
| Bivalirudin | major | |
| Boceprevir | major | |
| Bromfenac | major | |
| Cabozantinib | major | |
| Cangrelor | major | |
| Caplacizumab | major | |
| Carbamazepine | major | |
| Ceritinib | major | |
| Certolizumab pegol | major | |
| Chloroquine | major | |
| Cilostazol | major | |
| Cimetidine | major | |
| Cisapride | major | |
| Citalopram | major | |
| Cladribine | major |
Showing 40 of 100+.
Registered Products (16)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Daleubin | Tablet 50 mg | 60 tab | Sabbagh Drug Store | — |
| Daleubin | Tablet 70 mg | 60 tab | Sabbagh Drug Store | — |
| Daleubin | Tablet 20 mg | 60 tab | Sabbagh Drug Store | — |
| Dasatinib Dar Al Dawa | Tablet 50 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Dasatinib Dar AL Dawa | Tablet 20 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Dasatinib Dar Al Dawa | Tablet 80 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Dasatinib Dar Al Dawa | Tablet 100 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Dasatinib Dar Al Dawa | Tablet 70 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Dasatinib Dar Al-Dawa | Tablet 140 mg | 60 tab | / Dar Al Dawa Development and Investment Co Ltd/Jordan / General | — |
| Elpida | Tablet 140 mg | 30 tab | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Elpida | Tablet 70 mg | 60 tab | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Elpida | Tablet 50 mg | 60 tab | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Elpida | Tablet 20 mg | 60 tab | Hikma Pharmaceuticals Co.Ltd/Jordan | — |
| Sprycel | Tablet 20 mg | 60 tab | ORIENT DRUG STORE CO | — |
| Sprycel | Tablet 50 mg | 60 tab | ORIENT DRUG STORE CO | — |
| Sprycel | Tablet 70 mg | 60 tab | ORIENT DRUG STORE CO | — |