Voriconazole
JFDA label: Vfend Powder for Solution for Infusion
Mechanism of Action
Inhibitor of Lanosterol 14-alpha demethylase — Cytochrome P450 51 inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Lanosterol 14-alpha demethylase efficacy | INHIBITOR | ERG11 |
Indications
Approved
- Treatment of fungal infections
Off-label
- Acute myelogenous leukemia (prophylaxis of fungal infections)
- Allogeneic hematopoietic stem cell transplant (prophylaxis of fungal infections)
- Aspergillosis, invasive (prophylaxis during prolonged neutropenia)
- Aspergillosis, ocular
- Candidiasis, endophthalmitis
- Candidiasis, esophageal
- Candidiasis, intravascular infections
- Candidiasis, oropharyngeal (fluconazole-refractory)
- Coccidioidal meningitis (salvage therapy) (non-HIV infected patients)
- Coccidioidomycosis (treatment/chronic suppressive therapy) in HIV-infected patients (adolescents and adults)
- Empiric antifungal therapy (neutropenic fever)
- Fungal meningitis or osteoarticular infections (secondary to contaminated steroid products)
- Myelodysplastic Syndrome (prophylaxis of fungal infections)
- Talaromyces marneffei infection in HIV-infected patients (adolescents and adults)
Antimicrobial Spectrum
Expected / intrinsic spectrum (EUCAST breakpoints & labels) — not local resistance. Source: openfda-label.
Fungi
| Organism | Activity | MIC |
|---|---|---|
| Aspergillus flavus | Active | — |
| Aspergillus fumigatus | Active | — |
| Aspergillus niger | Active | — |
| Aspergillus terreus | Active | — |
| Candida albicans | Active | — |
| Candida glabrata | Active | — |
| Candida guilliermondii | Active | — |
| Candida krusei | Active | — |
| Candida lusitaniae | Active | — |
| Candida parapsilosis | Active | — |
| Candida tropicalis | Active | — |
| Fusarium solani | Active | — |
Class profile
| antifungalClass | Azole (extended-spectrum) |
|---|---|
| targetMolecule | Lanosterol 14-alpha-demethylase (CYP51) |
| isFungicidal | 0 |
| spectrumCandida | S (incl. non-albicans) |
| spectrumAspergillus | S (gold standard) |
| spectrumCryptococcus | S |
| spectrumDermatophytes | S |
| resistanceMechanisms | ERG11 mutations,Cyp51 mutations in Aspergillus (TR34/L98H),Efflux pumps |
| source | Pappas2016/Lass-Florl2011 |
Contraindications
Source: Lexicomp
- Hypersensitivity to voriconazole or any component of the formulation Absolute
- also avoid low dose [eg, 200 mg daily] dosing if possible), sirolimus, St John’s wort, terfenadine Documentation of allergenic cross-reactivity for imidazole antifungals is limited. However, because of similarities in chemical structure and/or pharmacologic actions, the possibility of cross-sensitivity cannot be ruled out with certainty Absolute
- coadministration with astemizole, barbiturates (long acting), carbamazepine, cisapride, efavirenz (≥400 mg daily), ergot derivatives (ergotamine and dihydroergotamine), pimozide, quinidine, rifampin, rifabutin, ritonavir (≥800 mg daily Absolute
Adverse Reactions
Cardiac disorders (1)
Common Tachycardia
Nervous system disorders (3)
Very Common Hallucination
Common Chills · headache
Hepatobiliary disorders (4)
Common cholestatic jaundice · Increased serum alkaline phosphatase · increased serum ALT · increased serum AST
Renal and urinary disorders (1)
Very Common Increased serum creatinine
Metabolism and nutrition disorders (1)
Common Hypokalemia
Gastrointestinal disorders (2)
Common Nausea · vomiting
Skin and subcutaneous tissue disorders (1)
Common Skin rash
Eye disorders (2)
Very Common Visual disturbance
Common Photophobia
General disorders and administration site conditions (1)
Common Fever
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Arrhythmias/QT prolongation
QT interval prolongation has been associated with voriconazole use; rare cases of arrhythmia (including torsade de pointes), cardiac arrest, and sudden death have been reported, usually in seriously ill patients with comorbidities and/or risk factors (eg, prior cardiotoxic chemotherapy, cardiomyopathy [especially with concomitant heart failure], electrolyte imbalance, or concomitant QTc-prolonging drugs). Also use with caution in patients with potentially proarrhythmic conditions (eg, congenital or acquired QT syndrome, sinus bradycardia, or preexisting symptomatic arrhythmias); correct electrolyte abnormalities (eg, hypokalemia, hypomagnesemia, hypocalcemia) prior to initiating and during therapy.
Dermatologic reactions
Rare cases of malignancy (melanoma, squamous cell carcinoma [SCC]) have been reported in patients with prior onset of severe photosensitivity reactions or exposure to standard dose long-term voriconazole therapy (in lung transplant recipients, SCC increased by ~6% per 60 days with a 28% absolute risk increase at 5 years [Singer 2012]). Other serious exfoliative cutaneous reactions, including Stevens-Johnson syndrome, toxic epidermal necrolysis, and erythema multiforme, have also been reported. Patients, including children, should avoid exposure to direct sunlight and should use protective clothing and high SPF sunscreen; may cause photosensitivity, especially with long-term use. Discontinue use in patients who develop an exfoliative cutaneous reaction or a skin lesion consistent with squamous cell carcinoma or melanoma. Periodic total body skin examinations should be performed, particularly with prolonged use. If phototoxic reactions occur, referral to a dermatologist and voriconazole discontinuation should be considered. If therapy is continued, dermatologic evaluation should be performed on a systematic and regular basis to allow early detection and management of premalignant lesions. Pediatric patients are at particular risk for phototoxicity (see Special Populations).
Hepatic toxicity
Serious (and rarely fatal) hepatic reactions (eg, hepatitis, cholestasis, fulminant failure) have been observed with voriconazole. In lung transplant recipients, median time to hepatic toxicity was 14 days with the majority occurring within 30 days of therapy initiation (Luong 2012). Use with caution in patients with serious underlying medical conditions (eg, hematologic malignancy); hepatic reactions have occurred in patients with no identifiable underlying risk factors. Liver dysfunction is usually reversible upon therapy discontinuation. Monitor serum transaminase and bilirubin at baseline and at least weekly for the first month of treatment. Monitoring frequency can then be reduced to monthly during continued use if no abnormalities are noted. If marked elevations occur compared to baseline, discontinue unless benefit/risk of treatment justifies continued use.
Infusion-related reactions
Anaphylactoid-type reactions including tachycardia, dyspnea, chest tightness, faintness, nausea, rash, pruritus, fever, sweating and flushing have been observed; symptoms have appeared immediately upon initiating the infusion. Stop infusion for severe reactions or as clinical presentation indicates.
Ocular effects
Visual changes, including blurred vision, changes in visual acuity, color perception, and photophobia, are commonly associated with treatment; postmarketing cases of optic neuritis and papilledema (lasting >1 month) have also been reported. Patients should be warned to avoid tasks which depend on vision, including operating machinery or driving. Changes are reversible on discontinuation following brief exposure/treatment regimens (≤28 days); reversibility following long-term administration has not been evaluated. If treatment continues >28 days, visual function (eg, acuity, visual field, color perception) should be monitored.
Renal toxicity
Acute renal failure has been observed in severely ill patients; use with caution in patients receiving concomitant nephrotoxic medications. Evaluate renal function (particularly serum creatinine) at baseline and periodically during therapy.
Skeletal effects
Fluorosis and/or periostitis may occur during long-term therapy. If patient develops skeletal pain and radiologic findings of fluorosis or periostitis, discontinue therapy.
Toxicity symptoms
Voriconazole demonstrates nonlinear pharmacokinetics. Dose modifications may result in unpredictable changes in serum concentrations and contribute to toxicity. For toxicity, the strongest correlations have been made between voriconazole trough concentrations and neurological and dermatological adverse events (Dolton 2012; Hamada 2012; Mitsani 2012; Park 2012; Soler-Palacin 2012). In these studies, increased toxicity was noted when trough concentrations exceeded threshold values. There are much less data supporting the existence between a cutoff threshold and hepatotoxicity. It is important to note that cutoff trough threshold values ranged widely among studies; however, an upper limit of Exserohilum rostratum in Reference Range section) (CDC 2012). Disease-related concerns:
Electrolyte abnormalities
Correct electrolyte abnormalities (eg, hypokalemia, hypomagnesemia, hypocalcemia) prior to initiating and during therapy.
Hepatic impairment
Use with caution; elevated liver function tests and clinical signs of liver damage, such as jaundice, have been associated with voriconazole. Adjustments to maintenance dosing is required in mild to moderate hepatic cirrhosis (Child-Pugh class A and B). In patients with severe hepatic insufficiency use only if the benefit outweighs the potential risk. Evaluate hepatic function (particularly liver function tests and bilirubin) at baseline and periodically during therapy.
Pancreatitis
Monitor pancreatic function in patients (children and adults) at risk for acute pancreatitis (eg, recent chemotherapy or hematopoietic stem cell transplantation). Pancreatitis has occurred in pediatric patients.
Renal impairment
Avoid the use of IV voriconazole in patients with renal impairment. See "Dosage forms specific issues: Injection: formulation." Evaluate renal function (particularly serum creatinine) at baseline and periodically during therapy. Concurrent drug therapy issues:
Drug-drug interactions
Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Pediatric pharmacokinetics
In pediatric patients, voriconazole pharmacokinetics are complex. In patients >14 years of age or 12 to 14 years and weighing >50 kg, data suggest that pharmacokinetics are similar to adults (Friberg 2012). In patients • Pediatric dermatologic reactions: Frequency of phototoxic reactions is higher in pediatric patients. Stringent photoprotective measures are necessary in children due to the risk of squamous cell carcinoma. In children experiencing photoaging injuries (eg, lentigines or ephelides), avoidance of sun and dermatologic follow-up are warranted even after treatment is discontinued. Dosage form specific issues:
Benzyl alcohol and derivatives
Some dosage forms may contain sodium benzoate/benzoic acid; benzoic acid (benzoate) is a metabolite of benzyl alcohol; large amounts of benzyl alcohol (≥99 mg/kg/day) have been associated with a potentially fatal toxicity (“gasping syndrome”) in neonates; the “gasping syndrome” consists of metabolic acidosis, respiratory distress, gasping respirations, CNS dysfunction (including convulsions, intracranial hemorrhage), hypotension, and cardiovascular collapse (AAP ["Inactive" 1997]; CDC 1982); some data suggests that benzoate displaces bilirubin from protein binding sites (Ahlfors 2001); avoid or use dosage forms containing benzyl alcohol derivative with caution in neonates. See manufacturer’s labeling.
Injection
Avoid/limit use of IV formulation in patients with moderate to severe renal impairment (CrCl • Oral: - Lactose: Tablets contain lactose; avoid administration in hereditary galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption. - Sucrose: Suspension contains sucrose; use caution with fructose intolerance, sucrase-isomaltase deficiency, or glucose-galactose malabsorption. Other warnings/precautions:
Monitoring
Evaluate renal function (particularly serum creatinine) and hepatic function (particularly liver function tests and bilirubin) at baseline and periodically during therapy.
Pregnancy & Lactation
Pregnancy
Voriconazole can cause fetal harm when administered to a pregnant woman. Voriconazole was teratogenic and embryotoxic in animal studies, and lowered plasma estradiol in animal models. Women of childbearing potential should use effective contraception during treatment. Should be used in pregnant woman only if benefit to mother justifies potential risk to the fetus.
Lactation
It is not known if voriconazole is excreted in breast milk. Due to the potential for serious adverse reactions in the nursing infant, the manufacturer recommends a decision be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of treatment to the mother.
Monitoring
| Efficacy | Fungal culture and species identification; minimum inhibitory concentration (MIC) where available; clinical response (temperature, imaging for invasive fungal disease) |
|---|---|
| Toxicity | LFTs (hepatotoxicity — azoles in particular); renal function; ECG for QT prolongation (azoles); drug levels if available (itraconazole, voriconazole) |
| Clinical pearl | Voriconazole levels are highly variable due to CYP2C19 polymorphism — TDM recommended (target trough 2–5 mg/L). Check for drug interactions with CYP3A4 substrates. |
| Counseling | Report visual disturbances (voriconazole), jaundice, or rash. Take azoles with food or as directed to optimise absorption. |
Chemistry & Properties
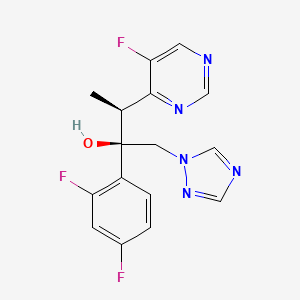
| Formula | C16H14F3N5O |
|---|---|
| Molecular weight | 349.32 g/mol |
| IUPAC name | (2R,3S)-2-(2,4-difluorophenyl)-3-(5-fluoropyrimidin-4-yl)-1-(1,2,4-triazol-1-yl)butan-2-ol |
| CAS | 137234-62-9 |
| PubChem CID | 71616 |
| InChIKey | BCEHBSKCWLPMDN-MGPLVRAMSA-N |
| logP | 2.18 (XLogP 1.5) |
| Polar surface area | 76.72 Ų |
| H-bond acceptors / donors | 6 / 1 |
| Drug-likeness (QED) | 0.76 |
| Lipinski violations | 0 |
SMILES
C[C@@H](c1ncncc1F)[C@](O)(Cn1cncn1)c1ccc(F)cc1FBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2B6 | Inhibitor | Ki 0.3687817782917156 µM |
| CYP2C19 | Inhibitor | Ki 5.099999999999999 µM |
| CYP2C9 | Inhibitor | Ki 2.800000000000001 µM |
| CYP3A4 | Inhibitor | IC₅₀ 13.000000000000005 µM |
| CYP3A4 | Substrate | — |
Transporters
BCRP (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)P-gp (Inhibitor)MDR1 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Abemaciclib | major | |
| Acalabrutinib | major | |
| Acetohexamide | major | |
| Aminolevulinic acid | major | |
| Anagrelide | major | |
| Apixaban | major | |
| Arsenic trioxide | major | |
| Astemizole | major | |
| Axitinib | major | |
| Bexarotene | major | |
| Bosutinib | major | |
| Brigatinib | major | |
| Budesonide | major | |
| Cabozantinib | major | |
| Ceritinib | major | |
| Chloroquine | major | |
| Chlorpropamide | major | |
| Cilostazol | major | |
| Cisapride | major | |
| Cobimetinib | major | |
| Copanlisib | major | |
| Crizotinib | major | |
| Cyclosporine | major | |
| Dasatinib | major | |
| Deflazacort | major | |
| Dicoumarol | major | |
| Docetaxel | major | |
| Dolasetron | major | |
| Elagolix | major | |
| Eliglustat | major | |
| Encorafenib | major | |
| Entrectinib | major | |
| Erythromycin | major | |
| Everolimus | major | |
| Fedratinib | major | |
| Fingolimod | major | |
| Fluticasone | major | |
| Fluticasone (nasal) | major | |
| Fostamatinib | major | |
| Gilteritinib | major |
Showing 40 of 100+.
Registered Products (9)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Voricet | Tablet Voriconazole 50.00 mg | 30 tab | Nabulsi Drug Store | 118.010 |
| Vecanzol | Vial 200 mg | 1 vial | MS PHARMA/JORDAN | — |
| Veron | Tablet 200 mg | 30 tab pack varies | Pharma International Company/ Jordan | — |
| Veron | Tablet 200 mg | 10 tab pack varies | Pharma International Company/ Jordan | — |
| Vfend Film Coated Tab | Film-Coated Tablet 200 mg | 30 tab pack varies | Khoury Drug Store | — |
| Vfend Film Coated Tab | Film-Coated Tablet 50 mg | 30 tab | Khoury Drug Store | — |
| Vfend Powder for Solution for Infusion | Infusion 200 mg | 1 vial pack varies | Khoury Drug Store | — |
| Voricet | Tablet Voriconazole 200.00 mg | 30 tab | Nabulsi Drug Store | — |
| vecanzol | Injection 40 mg/ml | 75 ml | United Pharmaceutical | — |