Ritonavir
JFDA label: Paxlovid
- Drug-drug interactions leading to potentially serious and/or life threatening reactions:
Mechanism of Action
Inhibitor of Human immunodeficiency virus type 1 protease — Human immunodeficiency virus type 1 protease inhibitor; Inhibitor of Cytochrome P450 3A — Cytochrome P450 3A inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Cytochrome P450 3A efficacy | INHIBITOR | |
| Human immunodeficiency virus type 1 protease efficacy | INHIBITOR | pol |
Indications
Approved
- HIV-1 infection
Off-label
- HIV-1 infection as a pharmacokinetic “booster” for other protease inhibitors
Class profile
| targetVirus | HIV-1 (boosting dose) |
|---|---|
| viralClass | Retrovirus (+ssRNA) |
| targetStep | Protease cleavage (PI) + CYP3A4 inhibition (pharmacokinetic booster) |
| resistanceBarrier | High (rarely used as antiretroviral alone) |
| crossResistance | Used as pharmacokinetic booster only |
| source | DHHS/AASLD/manufacturer-PIL |
Contraindications
Source: Lexicomp
- Additional contraindications (not in US labeling): Concurrent use with astemizole, bepridil, fusidic acid, rivaroxaban, voriconazole (regardless of ritonavir dose), salmeterol, terfenadine, vardenafil, or venetoclax (during dose initiation and the ramp-up phase) Absolute
- Hypersensitivity (eg, Stevens-Johnson syndrome, toxic epidermal necrolysis) to ritonavir or any component of the formulation Absolute
- coadministration with drugs that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening reactions or with potent CYP3A inducers where significantly reduced lopinavir plasma concentrations may be associated with the potential for loss of virologic response and possible resistance and cross-resistance (eg, alfuzosin, amiodarone, cisapride, colchicine [patients with renal and/or hepatic impairment], dronedarone, e Absolute
- eg, Revatio], simvastatin, St John's wort, triazolam, voriconazole [when ritonavir dose is ≥800 mg/day]) Absolute
Adverse Reactions
Cardiac disorders (5)
Very Common Flushing
Common Edema · hypertension · syncope · vasodilatation
Nervous system disorders (12)
Very Common dizziness · fatigue · Paresthesia
Common anxiety · confusion · depression · disturbance in attention · drowsiness · headache · insomnia · malaise · Peripheral neuropathy
Hepatobiliary disorders (1)
Very Common Increased gamma-glutamyl transferase
Renal and urinary disorders (1)
Common Polyuria
Blood and lymphatic system disorders (2)
Common Neutropenia · thrombocytopenia, increased serum ALT, hepatitis
Immune system disorders (1)
Common Hypersensitivity reaction
Metabolism and nutrition disorders (4)
Very Common Hypercholesterolemia · increased serum triglycerides
Common Increased uric acid · lipodystrophy
Gastrointestinal disorders (10)
Very Common abdominal pain · Diarrhea · dysgeusia dyspepsia · nausea · vomiting
Common Anorexia · flatulence · gastrointestinal hemorrhage · increased serum amylase · throat irritation
Skin and subcutaneous tissue disorders (4)
Very Common pruritus · Skin rash
Common Acne vulgaris · diaphoresis
Musculoskeletal and connective tissue disorders (4)
Very Common increased creatine phosphokinase · Musculoskeletal pain · weakness
Common Myalgia
Eye disorders (1)
Common Blurred vision
General disorders and administration site conditions (1)
Common Fever
Respiratory, thoracic and mediastinal disorders (3)
Very Common Cough · oropharyngeal pain
Common Pharyngitis
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
Hypersensitivity reactions
Protease inhibitors have been associated with a variety of hypersensitivity events (some severe), including rash, anaphylaxis (rare), angioedema, bronchospasm, erythema multiforme, toxic epidermal necrolysis, and/or Stevens-Johnson syndrome (rare). It is generally recommended to discontinue treatment if severe rash or moderate symptoms accompanied by other systemic symptoms occur.
Fat redistribution
May cause redistribution/accumulation of fat (eg, central obesity, buffalo hump, peripheral wasting, facial wasting, breast enlargement, cushingoid appearance).
Hepatotoxicity
May cause hepatitis, jaundice, and/or exacerbation of preexisting hepatic dysfunction (including fatalities); use with caution in patients with underlying hepatic disease, such as hepatitis B or C, cirrhosis, or those with high baseline transaminases; consider increased monitoring of transaminases in these patients.
Immune reconstitution syndrome
Patients may develop immune reconstitution syndrome resulting in the occurrence of an inflammatory response to an indolent or residual opportunistic infection during initial HIV treatment or activation of autoimmune disorders (eg, Graves’ disease, polymyositis, Guillain-Barré syndrome) later in therapy; further evaluation and treatment may be required.
Increased cholesterol
Increases in total cholesterol and triglycerides have been reported; screening should be done prior to therapy and periodically throughout treatment.
PR interval prolongation
Ritonavir has been associated with AV block (including second- and third-degree block) due to prolongation of PR interval; use caution with drugs that prolong the PR interval. Disease-related concerns:
Cardiovascular disease
Use with caution in patients with cardiomyopathy, ischemic heart disease, preexisting conduction abnormalities, or structural heart disease; may be at increased risk of conduction abnormalities (eg, second- or third-degree AV block).
Diabetes
Hyperglycemia, exacerbation of diabetes, diabetic ketoacidosis, and new-onset diabetes mellitus have been reported in patients receiving protease inhibitors. Consider monitoring for these conditions. In some patients who discontinued protease inhibitors, hyperglycemia persisted.
Hemophilia A or B
Use with caution in patients with hemophilia A or B; increased bleeding events, including spontaneous skin hematoma and hemarthrosis, during protease inhibitor therapy have been reported. Additional factor VIII may be needed.
Hepatic impairment
Use is not recommended in patients with severe hepatic impairment (Child-Pugh class C).
Pancreatitis
Use with caution in patients with increased triglycerides; pancreatitis has been observed (including fatalities). Monitor serum lipase and amylase, and for symptoms of nausea, vomiting, and/or abdominal pain. Temporary or permanent discontinuation may be clinically indicated. Concurrent drug therapy issues:
Drug-drug interactions
Coadministration of ritonavir with several classes of drugs, including antiarrhythmics, ergot alkaloids, and sedatives/hypnotics, may result in potentially serious and/or life-threatening adverse reactions due to possible effects of ritonavir on the hepatic metabolism of certain drugs. Review medications taken by patients prior to prescribing ritonavir or when prescribing other medications to patients already taking ritonavir. Potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information. Special populations:
Preterm neonates
Oral solution contains ethanol and propylene glycol; ethanol competitively inhibits propylene glycol metabolism; preterm infants may be at increased risk of toxicity due to decreased ability to metabolize propylene glycol. Postmarketing adverse reactions (cardiac toxicity, lactic acidosis, renal failure, CNS depression, respiratory complications, acute renal failure including fatalities) have been reported in preterm neonates receiving ritonavir-containing solutions. Do not use in neonates with a postmenstrual age (first day of mother's last menstrual period to birth plus elapsed time after birth) Dosage form specific issues:
Bioequivalence
Norvir tablets are not bioequivalent to Norvir capsules. Gastrointestinal side effects (eg, nausea, vomiting, abdominal pain, diarrhea) or paresthesias may be more common when patients are switching from the capsule to the tablet formulation due to a higher Cmax (26% increase) observed with the tablet formulation compared to the capsule. These side effects may decrease as therapy is continued.
Oral solution
The oral solution contains large amounts of ethanol (43.2%) and propylene glycol (26.57%). Healthcare providers should pay special attention to accurate calculation, measurement, and administration of dose. Overdose (or cumulative ethanol or propylene glycol content in medications) in a child may lead to lethal ethanol or propylene glycol toxicity.
Pregnancy & Lactation
Pregnancy
Ritonavir has a low level of transfer across the human placenta; no increased risk of overall birth defects has been observed following first trimester exposure according to data collected by the antiretroviral pregnancy registry. Maternal antiretroviral therapy (ART) may increase the risk of preterm delivery, although available information is conflicting possibly due to variability of maternal factors (disease severity; gestational age at initiation of therapy); however, maternal antiretroviral medication should not be withheld due to concerns of preterm birth. Information related to stillbirth, low birth weight, and small for gestational age infants is limited. Long-term follow-up is recommended for all infants exposed to antiretroviral medications; children who develop significant organ system abnormalities of unknown etiology (particularly of the CNS or heart) should be evaluated for potential mitochondrial dysfunction. Hyperglycemia, new onset of diabetes mellitus, or diabetic ket
Lactation
Ritonavir is present in breast milk. Maternal or infant antiretroviral therapy does not completely eliminate the risk of postnatal HIV transmission. In addition, multiclass-resistant virus has been detected in breastfeeding infants despite maternal therapy. Therefore, in the US, where formula is accessible, affordable, safe, and sustainable, and the risk of infant mortality due to diarrhea and respiratory infections is low, females with HIV infection should completely avoid breastfeeding to de
Monitoring
| Efficacy | Viral load (undetectable = success); CD4 count (HIV); hepatic enzymes and HBV/HCV DNA (hepatitis); clinical resolution of acute viral illness |
|---|---|
| Toxicity | Renal function (most antivirals are renally cleared); LFTs; resistance testing if virological failure; CBC |
| Clinical pearl | For HIV, undetectable viral load at 6 months predicts long-term treatment success. Resistance testing is mandatory at virological failure. |
| Counseling | Do not miss doses — even brief interruptions can cause viral rebound and resistance selection. Report any side effects early rather than stopping independently. |
Chemistry & Properties
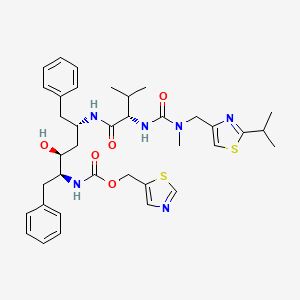
| Formula | C37H48N6O5S2 |
|---|---|
| Molecular weight | 720.96 g/mol |
| IUPAC name | 1,3-thiazol-5-ylmethyl N-[(2S,3S,5S)-3-hydroxy-5-[[(2S)-3-methyl-2-[[methyl-[(2-propan-2-yl-1,3-thiazol-4-yl)methyl]carbamoyl]amino]butanoyl]amino]-1,6-diphenylhexan-2-yl]carbamate |
| CAS | 155213-67-5 |
| PubChem CID | 392622 |
| InChIKey | NCDNCNXCDXHOMX-XGKFQTDJSA-N |
| logP | 5.91 (XLogP 6.0) |
| Polar surface area | 145.78 Ų |
| H-bond acceptors / donors | 9 / 4 |
| Drug-likeness (QED) | 0.11 |
| Lipinski violations | 2 |
SMILES
CC(C)c1nc(CN(C)C(=O)N[C@H](C(=O)N[C@@H](Cc2ccccc2)C[C@H](O)[C@H](Cc2ccccc2)NC(=O)OCc2cncs2)C(C)C)cs1Biology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | No |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP1A2 | Inhibitor | — |
| CYP1A2 | Substrate | — |
| CYP2B6 | Inhibitor | IC₅₀ 2.0000000000000004 µM |
| CYP2C19 | Inhibitor | IC₅₀ 12.700000000000012 µM |
| CYP2C8 | Inhibitor | — |
| CYP2C9 | Inhibitor | IC₅₀ 0.6905393808125321 µM |
| CYP2C9 | Substrate | — |
| CYP2D6 | Inhibitor | IC₅₀ 10.72380529476361 µM |
| CYP2D6 | Substrate | — |
| CYP3A | Moderate Inhibitor | — |
| CYP3A4 | Inhibitor | Ki 0.06861212035840819 µM |
| CYP3A4 | Substrate | — |
Receptor binding (top 3)
| Target | Action | Affinity |
|---|---|---|
| CYP3A4 (CYP3A4) | Inhibitor | pKi 7.0 |
| CYP3A5 (CYP3A5) | Inhibitor | pKi 6.9 |
| UDP glucuronosyltransferase family 1 member A1 (UGT1A1) | Inhibitor | pIC50 5.8 |
Transporters
BCRP (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MATE1 (Inhibitor)MATE2 (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)NTCP (Inhibitor)OAT (Inhibitor)OAT1 (Inhibitor)OATP (Inhibitor)OATP1A2 (Inhibitor)OATP1B (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)OATP2B1 (Inhibitor)OCT1 (Inhibitor)OCT2 (Inhibitor)OCT3 (Inhibitor)OCTN2 (Inhibitor)P-gp (Inhibitor)MDR1 (Substrate)MRP1 (Substrate)MRP2 (Substrate)MRP3 (Substrate)OATP (Substrate)OCT2 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Abemaciclib | major | |
| Acalabrutinib | major | |
| Apalutamide | major | |
| Apixaban | major | |
| Artemether | major | |
| Astemizole | major | |
| Axitinib | major | |
| Betrixaban | major | |
| Bexarotene | major | |
| Bosutinib | major | |
| Brigatinib | major | |
| Budesonide | major | |
| Cabozantinib | major | |
| Ceritinib | major | |
| Cilostazol | major | |
| Cisapride | major | |
| Clopidogrel | major | |
| Cobimetinib | major | |
| Copanlisib | major | |
| Crizotinib | major | |
| Cyclosporine | major | |
| Dasatinib | major | |
| Deflazacort | major | |
| Disulfiram | major | |
| Docetaxel | major | |
| Edoxaban | major | |
| Elagolix | major | |
| Eliglustat | major | |
| Eluxadoline | major | |
| Encorafenib | major | |
| Entrectinib | major | |
| Enzalutamide | major | |
| Erythromycin | major | |
| Everolimus | major | |
| Fedratinib | major | |
| Fluticasone | major | |
| Fluticasone (nasal) | major | |
| Fostamatinib | major | |
| Gilteritinib | major | |
| Glasdegib | major |
Showing 40 of 100+.
Registered Products (1)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Paxlovid | Tablet 100 mg, 150 mg | 30 tab | Khoury Drug Store | — |