Itraconazole
JFDA label: CONAZOLE CAP
- Congestive heart failure:
- Drug interactions:
Mechanism of Action
Inhibitor of Lanosterol 14-alpha demethylase — Cytochrome P450 51 inhibitor
| Target | Action | Gene / class |
|---|---|---|
| Lanosterol 14-alpha demethylase efficacy | INHIBITOR | ERG11 |
Indications
Approved
- Aspergillosis (capsules)
- Blastomycosis (capsules)
- Canadian labeling
- Candidiasis, oral and/or esophageal
- Capsules
- Chromomycosis
- Dermatomycoses
- Histoplasmosis (capsules)
- Onychomycosis
- Oropharyngeal/Esophageal candidiasis (oral solution)
- Paracoccidioidomycosis
- Sporotrichosis
- Tablets
Off-label
- Additional off-label uses
- Candidiasis, vulvo-vaginal in HIV-infected patients (adolescents and adults)
- Coccidioidal meningitis in HIV-infected patients (adolescents and adults)
- Coccidioidal pneumonia in HIV-infected patients (adolescents and adults)
- Coccidioidomycosis (non-HIV infected)
- Cryptococcosis in HIV-infected patients (adults and adolescents)
- Histoplasmosis (primary prophylaxis/long-term suppression therapy) in HIV-infected patients (adolescents and adults)
- Microsporidiosis, disseminated in HIV-infected patients (adolescents and adults)
- Penicilliosis in HIV-infected patients (adolescents and adults)
Antimicrobial Spectrum
Expected / intrinsic spectrum (EUCAST breakpoints & labels) — not local resistance. Source: openfda-label.
Fungi
| Organism | Activity | MIC |
|---|---|---|
| Aspergillus flavus | Active | — |
| Aspergillus fumigatus | Active | — |
| Blastomyces dermatitidis | Active | — |
| Histoplasma capsulatum | Active | — |
| Histoplasma duboisii | Active | — |
Class profile
| antifungalClass | Azole |
|---|---|
| targetMolecule | Lanosterol 14-alpha-demethylase (CYP51) |
| isFungicidal | 0 |
| spectrumCandida | S |
| spectrumAspergillus | S (but not reliable) |
| spectrumCryptococcus | S |
| spectrumDermatophytes | S |
| resistanceMechanisms | ERG11 mutations,Efflux pumps,Poor GI absorption (capsule form) |
| source | Pappas2016/Lass-Florl2011 |
Contraindications
Source: Lexicomp · Curated
- Additional contraindications (not in US labeling): Concurrent administration with domperidone, eletriptan, fesoterodine in patients with moderate to severe renal or hepatic impairment, or solifenacin in patients with severe renal impairment or moderate to severe hepatic impairment (capsule, oral solution) Absolute
- Concomitant use with CYP3A4 substrates that can cause serious arrhythmias (e.g., cisapride, pimozide, quinidine) Absolute
- Concurrent administration with the following drugs (none of which are available in Canada): Astemizole, bepridil, halofantrine, ivabradine, lercanidipine, levacetylmethadol, mizolastine, telithromycin (in patients with severe renal or hepatic impairment), sertindole, terfenadine (capsule, oral solution) Absolute
- Hypersensitivity to itraconazole or any component of the formulation Absolute
- coadministration with eliglustat in patients who are poor or intermediate metabolizers of CYP2D6 and in patients taking strong or moderate CYP2D6 inhibitors Absolute
- concurrent administration with avanafil, cisapride, disopyramide, dofetilide, dronedarone, eplerenone, ergot derivatives, felodipine, irinotecan, isavuconazole, ivabradine, lomitapide, lovastatin, lurasidone, methadone, midazolam (oral), naloxegol, nisoldipine, pimozide, quinidine, ranolazine, simvastatin, ticagrelor, or triazolam Absolute
- concurrent administration with colchicine, fesoterodine, or solifenacin in patients with varying degrees of renal or hepatic impairment Absolute
- treatment of dermatomycosis (tinea pedis, tinea cruris, tinea corporis, pityriasis versicolor) in women who are pregnant or intend to become pregnant (capsule) Absolute
- treatment of onychomycosis (or other non-life-threatening indications) in patients with evidence of ventricular dysfunction, such as congestive heart failure (CHF) or a history of CHF Absolute
- treatment of onychomycosis in women who are pregnant or contemplating pregnancy Absolute
Adverse Reactions
Cardiac disorders (3)
Common chest pain · Edema · hypertension
Nervous system disorders (8)
Common abnormal dreams · anxiety · depression · dizziness · fatigue · Headache · malaise · pain
Hepatobiliary disorders (2)
Common Abnormal hepatic function tests · increased liver enzymes
Renal and urinary disorders (2)
Common Cystitis · urinary tract infection
Metabolism and nutrition disorders (2)
Common Hypertriglyceridemia · hypokalemia
Gastrointestinal disorders (11)
Common abdominal pain · aphthous stomatitis · constipation · dyspepsia · flatulence · gastritis · gastroenteritis · gastrointestinal disease · gingivitis · increased appetite · Vomiting
Skin and subcutaneous tissue disorders (3)
Common diaphoresis · pruritus · Skin rash
Musculoskeletal and connective tissue disorders (3)
Common Bursitis · myalgia · tremor
Infections and infestations (1)
Common Herpes zoster
General disorders and administration site conditions (1)
Common Fever
Other (2)
Very Common Gastrointestinal: Diarrhea · nausea
Respiratory, thoracic and mediastinal disorders (7)
Common cough · dyspnea · pharyngitis · pneumonia · Rhinitis · sinusitis · upper respiratory tract infection
Dosing
Source: Lexicomp
Warnings & Precautions
Source: Lexicomp
CNS depression
May cause CNS depression, which may impair physical or mental abilities; patients must be cautioned about performing tasks that require mental alertness (eg, operating machinery, driving)
Hearing loss
Transient or permanent hearing loss has been reported. Quinidine (a contraindicated drug) was used concurrently in several of these cases. Hearing loss usually resolves after discontinuation, but may persist in some patients.
Heart failure
Negative inotropic effects have been observed following intravenous administration. Discontinue or reassess use if signs or symptoms of heart failure (HF) occur during treatment. CHF has been reported, particularly in patients receiving a total daily oral dose of 400 mg. Use with caution in patients with risk factors for HF (COPD, renal failure, edematous disorders, ischemic or valvular disease). Discontinue treatment if signs or symptoms of heart failure develop. In a scientific statement from the American Heart Association, itraconazole has been determined to be an agent that may exacerbate underlying myocardial dysfunction (magnitude: major); may consider use when treating life-threatening fungal infections (AHA [Page 2016]).
Hepatotoxicity
Rare cases of serious hepatotoxicity (including liver failure and death) have been reported (including some cases occurring within the first week of therapy); hepatotoxicity was reported in some patients without preexisting liver disease or risk factors. Discontinue treatment if signs or symptoms of hepatotoxicity develop.
Hypersensitivity
Use caution in patients with a history of hypersensitivity to other azoles.
Neuropathy
Discontinue if signs or symptoms of neuropathy occur during treatment. Disease-related concerns:
Cystic fibrosis
Large differences in itraconazole pharmacokinetic parameters have been observed in cystic fibrosis patients receiving the oral solution; if a patient with cystic fibrosis does not respond to therapy, alternate therapies should be considered.
Hepatic impairment
Use with caution in patients with hepatic impairment; monitor liver function closely. Not recommended for use in patients with active liver disease, elevated liver enzymes, or prior hepatotoxic reactions to other drugs unless the expected benefit exceeds the risk of hepatotoxicity.
Onychomycosis
Use is contraindicated for treatment of onychomycosis in patients with ventricular dysfunction such as heart failure (HF) or a history of HF. Cases of HF, peripheral edema, and pulmonary edema have occurred in this patient population. Due to potential toxicity, the manufacturer recommends confirmation of diagnosis testing of nail specimens prior to treatment of onychomycosis.
Renal impairment
Use with caution in patients with renal impairment; limited information is available; dosage adjustment may be needed. Concurrent drug therapy issues:
Drug-drug interactions
Additional potentially significant interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Consult drug interactions database for more detailed information.
High potential for interactions
Life-threatening cardiac dysrhythmias and/or sudden death have occurred in patients taking CYP 3A inhibitors such as cisapride, pimozide, methadone or quinidine. [US Boxed Warning]: Coadministration with itraconazole can cause elevated plasma concentrations of certain drugs and can lead to QT prolongation and ventricular tachyarrhythmias, including torsades de pointes. Coadministration with methadone, disopyramide, dofetilide, dronedarone, quinidine, isavuconazole, ergot alkaloids, irinotecan, lurasidone, oral midazolam, pimozide, triazolam, felodipine, nisoldipine, ivabradine, ranolazine, eplerenone, cisapride, naloxegol, lomitapide, lovastatin, simvastatin, avanafil, ticagrelor and, in subjects with varying degrees of renal or hepatic impairment, colchicine, fesoterodine, and solifenacin is contraindicated. Coadministration with eliglustat is contraindicated in poor or intermediate metabolizers of CYP2D6 and in patients taking strong or moderate CYP2D6 inhibitors. Dosage form specific issues:
Oral capsules/tablets
Absorption of itraconazole capsules is reduced when gastric acidity is reduced (eg, achlorhydria, acid suppressive therapy) administer capsules or tablets with an acidic beverage (eg, non-diet cola) in patients with reduced gastric acidity and separate administration from acid suppressive therapy (refer to drug interactions section). Monitor for response.
Oral solution
Only the oral solution has proven efficacy in oral/esophageal candidiasis; mucosal exposure may vary between the oral solution and capsules. Initiation of treatment with oral solution is not recommended in patients at immediate risk for systemic candidiasis (eg, patients with severe neutropenia).
Product interchangeability
Due to differences in bioavailability, oral capsules and oral solution cannot be used interchangeably.
Propylene glycol
Some dosage forms may contain propylene glycol; large amounts are potentially toxic and have been associated hyperosmolality, lactic acidosis, seizures and respiratory depression; use caution (AAP 1997; Zar 2007). Other warnings/precautions:
Appropriate use
Itraconazole should NOT be used for voriconazole-refractory aspergillosis because the same antifungal and/or resistance mechanism(s) may be shared by both agents.
Pregnancy & Lactation
Pregnancy
Dose-related adverse events were observed in animal reproduction studies at maternally toxic doses. Itraconazole exposure during the first trimester of pregnancy has not been associated with congenital malformations; however, an increase in the rate of early fetal loss has been reported (Bar-Oz 2000; DeSantis 2009; Molgaard-Nielsen 2013). Congenital abnormalities (eg, skeletal, genitourinary tract, cardiovascular and ophthalmic malformations, chromosomal abnormalities, and multiple malformations) have been reported during postmarketing surveillance; however, a causal relationship has not been established. Itraconazole is approved for the treatment of various fungal infections; however, when treatment of a systemic fungal infection is needed in pregnant women, itraconazole should be avoided, especially during the first trimester (Chapman 2008; Galgiani 2005; HHS [OI adult 2017]; Pappas 2016; Perfect 2010; Wheat 2007). Due to the potential risk of congenital malformations, the manufa
Lactation
Itraconazole is present in breast milk. According to the manufacturer, the decision to continue or discontinue breastfeeding during therapy should take into account the risk of infant exposure, the benefits of breastfeeding to the infant, and benefits of treatment to the mother (Sporanox prescribing information 2015). In the United States, where formula is accessible, affordable, safe, and sustainable, and the risk of infant mortality due to diarrhea and respiratory infections is low, complete
Monitoring
| Efficacy | Fungal culture and species identification; minimum inhibitory concentration (MIC) where available; clinical response (temperature, imaging for invasive fungal disease) |
|---|---|
| Toxicity | LFTs (hepatotoxicity — azoles in particular); renal function; ECG for QT prolongation (azoles); drug levels if available (itraconazole, voriconazole) |
| Clinical pearl | Voriconazole levels are highly variable due to CYP2C19 polymorphism — TDM recommended (target trough 2–5 mg/L). Check for drug interactions with CYP3A4 substrates. |
| Counseling | Report visual disturbances (voriconazole), jaundice, or rash. Take azoles with food or as directed to optimise absorption. |
Chemistry & Properties
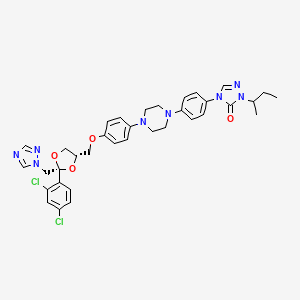
| Formula | C35H38Cl2N8O4 |
|---|---|
| Molecular weight | 705.65 g/mol |
| IUPAC name | 2-butan-2-yl-4-[4-[4-[4-[[(2R,4S)-2-(2,4-dichlorophenyl)-2-(1,2,4-triazol-1-ylmethyl)-1,3-dioxolan-4-yl]methoxy]phenyl]piperazin-1-yl]phenyl]-1,2,4-triazol-3-one |
| CAS | 84625-61-6 |
| PubChem CID | 55283 |
| InChIKey | VHVPQPYKVGDNFY-UHFFFAOYSA-N |
| logP | 5.58 (XLogP 5.7) |
| Polar surface area | 104.7 Ų |
| H-bond acceptors / donors | 12 / 0 |
| Drug-likeness (QED) | 0.17 |
| Lipinski violations | 3 |
SMILES
CCC(C)n1ncn(-c2ccc(N3CCN(c4ccc(OCC5COC(Cn6cncn6)(c6ccc(Cl)cc6Cl)O5)cc4)CC3)cc2)c1=OBiology & Pharmacokinetics
Pharmacokinetics
| BBB penetrant | Yes (logBB -0.64) |
|---|
Enzyme interactions
| Enzyme | Role | Detail |
|---|---|---|
| CYP2B6 | Inhibitor | — |
| CYP3A4 | Inhibitor | IC₅₀ 0.09919290669286347 µM |
| CYP3A4 | Substrate | — |
Transporters
BCRP (Inhibitor)BCRP (Inhibitor)BSEP (Inhibitor)BSEP (Inhibitor)MDR1 (Inhibitor)MRP1 (Inhibitor)MRP2 (Inhibitor)MRP3 (Inhibitor)MRP4 (Inhibitor)NTCP (Inhibitor)OATP1B1 (Inhibitor)OATP1B1 (Inhibitor)OATP1B3 (Inhibitor)OATP1B3 (Inhibitor)OATP2B1 (Inhibitor)P-gp (Inhibitor)MDR1 (Substrate)OATP1B1 (Substrate)OATP1B3 (Substrate)OATP2B1 (Substrate)OCT1 (Substrate)P-gp (Substrate)
Drug–drug interactions (100+, DDInter)
| Interacting drug | Severity | Management |
|---|---|---|
| Abemaciclib | major | |
| Acalabrutinib | major | |
| Apixaban | major | |
| Artemether | major | |
| Astemizole | major | |
| Axitinib | major | |
| Betrixaban | major | |
| Bosutinib | major | |
| Brigatinib | major | |
| Budesonide | major | |
| Cabozantinib | major | |
| Ceritinib | major | |
| Cilostazol | major | |
| Cisapride | major | |
| Cobimetinib | major | |
| Copanlisib | major | |
| Crizotinib | major | |
| Cyclosporine | major | |
| Dasatinib | major | |
| Deflazacort | major | |
| Docetaxel | major | |
| Edoxaban | major | |
| Elagolix | major | |
| Eliglustat | major | |
| Encorafenib | major | |
| Entrectinib | major | |
| Erythromycin | major | |
| Everolimus | major | |
| Fedratinib | major | |
| Fluticasone | major | |
| Fluticasone (nasal) | major | |
| Fostamatinib | major | |
| Gilteritinib | major | |
| Glasdegib | major | |
| Halofantrine | major | |
| Hydrocodone | major | |
| Ibrutinib | major | |
| Irinotecan | major | |
| Irinotecan (liposomal) | major | |
| Ivacaftor | major |
Showing 40 of 100+.
Registered Products (5)
| Brand | Form / strength | Pack | Agent | Citizen (JOD) |
|---|---|---|---|---|
| Itrazol | Tablet 100 mg | 4 tab pack varies | Ibn Rushd Drug Store | 1.630 |
| CONAZOLE CAP | Capsule 100 mg | 4 cap | Jordan Sweden Medical & Sterilization Co. | 1.950 |
| Itrazol | Capsule 100 mg | 15 cap pack varies | Ibn Rushd Drug Store | 5.770 |
| Conazole Cap. | Capsule 100 mg | 15 cap | Jordan Sweden Medical & Sterilization Co. | 6.900 |
| Sporanox Caps | Capsule 100 mg | 15 cap | Telegraph Drug Store | 7.830 |